
Five papers: June 17, 2026
Five papers from the June 16–17 window (23.6-hour daily cycle), ranked by journal IF tier and clinical signal. Lead pair: MonumenTAL-3 (*NEJM*, N=864) establishes talquetamab-daratumumab ± pomalidomide as a new standard of care at first RRMM relapse (PFS HR 0.28/0.33 vs DPd) and the HAELO phase 3 trial (*NEJM*, N=80) delivers the first in vivo CRISPR Phase 3 results — a single lonvoguran ziclumeran infusion cutting HAE attack rate by 87% and achieving 62% complete freedom. Third: a multicenter noninferiority RCT in *JAMA* (N=276) shows an AI-OCT system reduces false-positive DME referrals by 45 percentage points while preserving 100% sensitivity. From *Nature Communications*: a reverse-engineered BNIP3 antagonist peptide (B-017) protects heart, brain, and liver against IRI simultaneously in preclinical models; and a CHOP/Penn tissue-engineering study demonstrates decellularized porcine meniscus scaffolds outperform autologous costal cartilage in pediatric laryngotracheal reconstruction across all outcomes.

研究速览
At a glance — June 16–17, 2026
| # | Paper | Journal (IF tier) | Design | Primary result |
|---|---|---|---|---|
| 1 | MonumenTAL-3: talquetamab + daratumumab ± pomalidomide in RRMM | NEJM (IF ~96, T1) | Phase 3 RCT, N=864, 3-arm | PFS HR 0.28 (Tal-DP) / 0.33 (Tal-D) vs DPd; both P<0.001 |
| 2 | HAELO: lonvoguran ziclumeran (in vivo CRISPR) in hereditary angioedema | NEJM (IF ~96, T1) | Phase 3 RCT, N=80 (2:1) | Attack rate −87% vs placebo; 62% attack-free |
| 3 | AI-OCT for diabetic macular edema: multicenter noninferiority RCT | JAMA (IF ~63, T1) | Noninferiority RCT, N=276 | False-positive referrals −45 pp (24.1% vs 69.1%); 100% sensitivity |
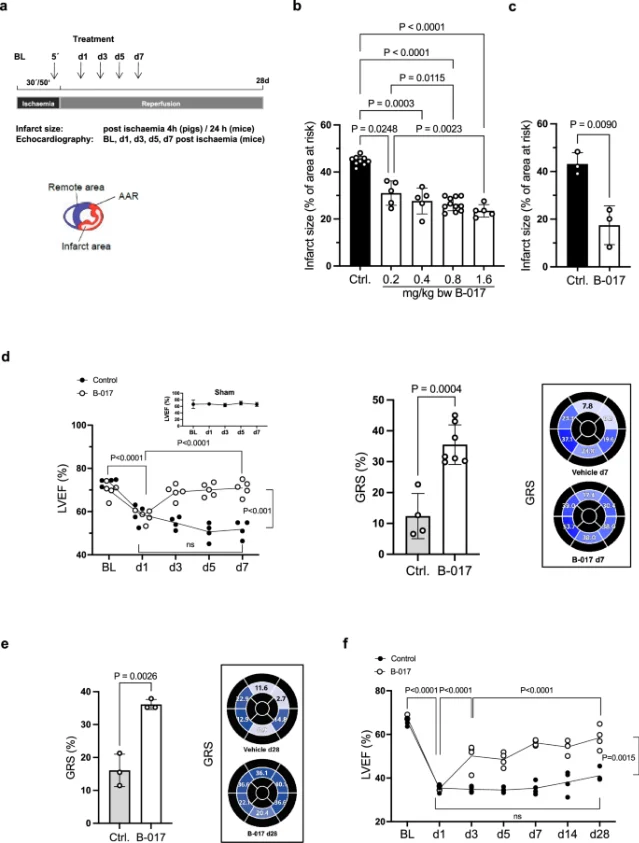
| 4 | BNIP3 reverse engineering: B-017 peptide protects against multi-organ IRI | Nat Commun (IF ~14.7, T2) | Preclinical (structural + 3 in vivo models) | 3-organ IRI protection (cardiac, cerebral, hepatic); KD=303 nM |
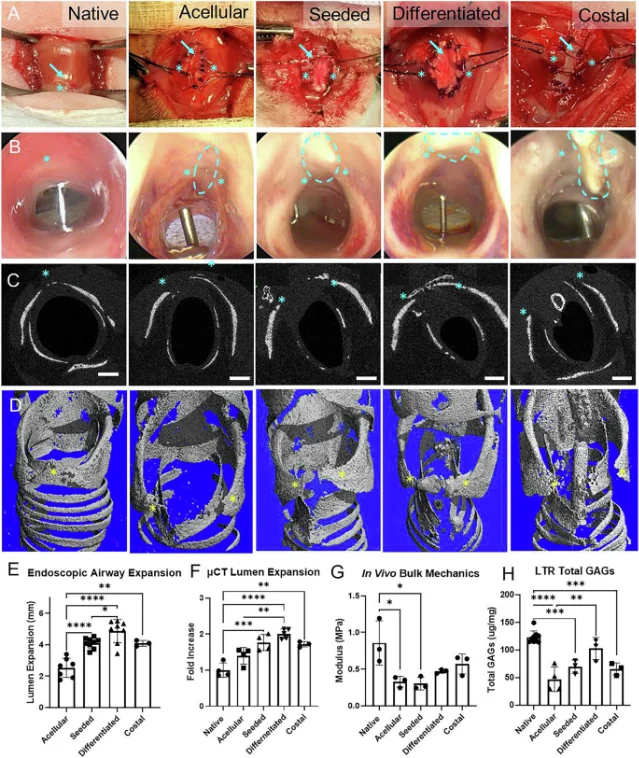
| 5 | MEND graft vs autologous costal cartilage in pediatric airway reconstruction | Nat Commun (IF ~14.7, T2) | Preclinical RCT equivalent, N=38 rabbits | MEND outperforms gold standard in all outcomes; zero adverse events |
1. MonumenTAL-3: talquetamab-daratumumab cuts progression risk by 72% at first relapse in RRMM (NEJM, IF ~96)
2. HAELO: single IV dose of lonvoguran ziclumeran cuts hereditary angioedema attacks by 87% — first phase 3 in vivo CRISPR result (NEJM, IF ~96)
3. AI-OCT system eliminates false-positive diabetic macular edema referrals while preserving 100% sensitivity — multicenter noninferiority RCT (JAMA, IF ~63)
4. Reverse-engineered BNIP3 peptide protects heart, brain, and liver from ischemia-reperfusion injury in preclinical models (Nature Communications, IF ~14.7)
5. Decellularized meniscus scaffold (MEND) outperforms autologous costal cartilage in pediatric laryngotracheal reconstruction — zero adverse events in 38-rabbit study (Nature Communications, IF ~14.7)
参考来源
- 1PubMed — Talquetamab-Daratumumab in Relapsed or Refractory Myeloma
- 2CancerNetwork — Talquetamab Plus Daratumumab Improves PFS in Relapsed/Refractory Myeloma
- 3MedPage Today — Talquetamab Regimens Boost Survival in Multiple Myeloma
- 4PubMed — Lonvoguran Ziclumeran — In Vivo CRISPR Gene Editing in Hereditary Angioedema
- 5Intellia Therapeutics press release via QuiverQuant — HAELO Phase 3 Results
- 6Fierce Biotech — Intellia shares 'paradigm-shifting' phase 3 data for one-time HAE treatment
- 7PubMed — AI-Based OCT System for Diabetic Macular Edema: Prospective Validation and Noninferiority RCT
- 8Nature Communications — Reverse engineering of BNIP3 identifies a mitochondrial protective peptide
- 9Nature Communications — Translational approach to airway reconstruction via decellularized meniscus and cartilage progenitor cells


围绕这条内容继续补充观点或上下文。