
2026/6/21 · 9:33
Sleep Research Digest Jun 14–21 2026
SLEEP 2026 (Baltimore, Jun 14–17) produced a wave of findings led by a 1.07-million-veteran COMISA study showing combined insomnia and sleep apnea multiplies type 2 diabetes risk 6.2×. Two preprints from 60K+ UK Biobank and 81K+ Apple Watch datasets independently converged on sleep regularity outperforming duration as a disease predictor. Oura published three validated PPG algorithm results; WHOOP reported a Weill Cornell slow-wave sleep / Alzheimer's cognition correlation; Matthew Walker's EP140 reframed insomnia as physiological hyperarousal. The actionable insight: measure and minimize your sleep midpoint variability before optimizing any other sleep variable.

研究速览
SLEEP 2026 (Baltimore, June 14–17) dominated a week that also produced two converging preprints making the same uncomfortable argument: in a dataset of 60,000+ people tracked for nearly a decade, irregular sleep predicted disease risk for 131 conditions — more than double the number flagged by simply sleeping too little. A second preprint from Apple's 81,000-person dataset found the same direction. Sleep regularity is not a wellness talking point anymore; it is pulling ahead of sleep duration as the stronger disease predictor in the two largest naturalistic datasets yet published on the question.
The conference added its own weight: a study of 1.07 million veterans found that having both insomnia and sleep apnea simultaneously multiplies type 2 diabetes risk by 6.2x — well beyond the risk of either disorder alone. Oura published three validated PPG algorithm results. WHOOP published a Weill Cornell study connecting wrist-worn slow-wave sleep data to cognitive test performance in people at genetic risk for Alzheimer's disease. And Matthew Walker released Episode 140 on why the "tired but wired" pattern at 2 a.m. is a physiological overspeed problem, not a sleep deficit.
SLEEP 2026 conference highlights
40th Annual Meeting of the Associated Professional Sleep Societies (AASM + SRS), Baltimore, June 14–17, 2026. ~5,000 attendees. Abstracts published in SLEEP, DOI prefix 10.1093/sleep/zsag091.
Veterans with both insomnia and sleep apnea: 6.2x diabetes risk
The largest study at the conference by sample size tracked 1,074,113 U.S. veterans (mean age 33, 12% women) with no baseline sleep disorders or diabetes, using ICD codes and time-varying exposure models. 1
The results: insomnia alone raised diabetes risk by 41%; sleep apnea alone raised it by more than 5x in men and roughly 4x in women. But COMISA (co-morbid insomnia and sleep apnea, occurring together) produced a hazard ratio of 6.2x overall — 6.5x in men, 4.7x in women — after adjusting for BMI, smoking, hypertension, hyperlipidemia, psychiatric conditions, and substance use.
Lead author Karam Al Jumaily, MD (Yale): "What was particularly striking was that these associations remained significant even after accounting for a broad range of demographic, metabolic, psychiatric, and behavioral risk factors." 1
The mechanism is not settled, but COMISA creates a bidirectional loop: fragmented sleep from OSA worsens insulin sensitivity, while arousal hyperactivation from insomnia keeps cortisol and sympathetic tone elevated — a combination that presumably hits glucose regulation harder than either disorder alone.
Daytime sleepiness + slow sleep onset triples hypertension risk
A Penn State Adult Cohort study (n=1,741 adults, 8-hour in-lab PSG) found that excessive daytime sleepiness (EDS) alone was associated with 52% higher odds of prevalent hypertension and 74% higher odds of incident hypertension. 2
The more striking number: when EDS co-occurred with objectively measured sleep-onset latency ≥30 minutes on PSG, odds of incident hypertension more than tripled. Among the 786 participants without baseline hypertension, the combination was the dominant risk signal at 7.5-year follow-up, adjusted for sex, age, BMI, race, smoking, caffeine, alcohol, diabetes, depression, OSA severity, total sleep time, and WASO.
Neither EDS alone nor prolonged SOL alone produced the same amplified effect — it required both. Lead author Alexandros Vgontzas, MD (Penn State): "These findings suggest that evaluating excessive daytime sleepiness should extend beyond screening for sleep apnea alone." 2

Women with OSA report more symptoms than men at the same AHI
A study of 502 adults (287 men, 202 women) with moderate-to-severe OSA initiating CPAP found that women scored significantly worse than men on 10 symptom domains — nocturia, headache, nightmares, sleep disturbance, daytime impairment, anxiety, anger, fatigue, depression, and cognitive function — despite nearly identical mean apnea-hypopnea index (AHI) scores (women: 36 events/hr; men: 40 events/hr). 3
No sex differences appeared on snoring, nocturnal gasping, or Epworth Sleepiness Scale scores — the classical symptoms that current diagnostic algorithms are calibrated around. Lead author Stuti Vaidya (University of Pittsburgh): "Current algorithms used by clinicians to diagnose and treat patients with obstructive sleep apnea continue to focus on classical symptoms and do not consider the broader range of symptoms women may experience." 3
The practical implication: women whose primary complaint is fatigue, depression, or cognitive fog — rather than snoring — may be waiting years for an OSA referral that the current system is not designed to trigger.
Rural patients: 25% lower odds of OSA referral
Among 25,917 high-risk patients in the Cleveland Clinic Health System (Ohio and Florida, 2017–2024), referral rates for sleep apnea evaluation were 15% in rural patients versus 20% in urban patients. After full adjustment for age, sex, race, BMI, insurance type, state, and Area Deprivation Index, rural patients had 25% lower odds of referral. 4
The rural patients who did get referred had higher median BMI and greater socioeconomic disadvantage than their urban counterparts — meaning the rural patients who made it through the referral filter were already more visibly ill.
Teen bedtime phone use feeds a same-night cascade
A passive smartphone monitoring study (n=230 U.S. adolescents, ~17 days of tracking via the RealityMeter app) found that on nights when teens used their phone an additional 20 minutes before bed, they used it for 8–9 more minutes after midnight that same night. 5
Teens averaged 46 minutes of late-night smartphone use per night in this sample. The within-person design matters here: it's not just that heavy phone users sleep less (a selection effect) — the same person uses their phone more at night when they use it more just before bed.

Oveporexton Phase 3: first orexin agonist nears FDA approval
Takeda's oveporexton (TAK-861), an oral orexin receptor 2 (OX2R) agonist, completed two Phase 3 trials in narcolepsy type 1 (NT1): FirstLight (n=168) and RadiantLight (n=105) across 19 countries. 6 At 12 weeks, daily functioning improved across all six FINI domains (p<0.001); roughly 70% of patients on any dose reported no significant cognitive difficulties versus ~15% on placebo; REM architecture shifted toward healthy controls; most patients reported no hallucinations or sleep paralysis.
If approved, oveporexton would be the first drug in its class — an orexin agonist restoring the neurochemical that NT1 patients lose when their hypocretin-producing neurons are destroyed. The FDA accepted the NDA with Priority Review; PDUFA goal date is Q3 2026. Emmanuel Mignot, MD, PhD (Stanford, principal investigator on FirstLight) called the results capable of "shifting disease management beyond incremental symptom relief." 6
Jazz Pharmaceuticals and Inspire Medical Systems also presented substantive datasets at SLEEP 2026. Jazz's DUET study found a mean of 41.8–42.1 days to reach a stable Xywav (low-sodium oxybate) dose; EHR data across Xywav initiators showed decreased non-HDL cholesterol and triglycerides, with decreased systolic blood pressure in patients switching from high-sodium formulations. 7 Inspire Medical's target trial emulation (4,388 matched patients) found hypoglossal nerve stimulation therapy associated with reduction in 8 of 9 major adverse cardiovascular event diagnoses versus untreated controls, with 93% device adherence at 90 days versus 56% for CPAP. 8
Quick-scan: peer-reviewed papers, June 14–21, 2026
| Paper | Journal | Design | N | Top result |
|---|---|---|---|---|
| Sleep regularity outweighs duration as disease predictor | medRxiv (preprint) | UK Biobank prospective, 9.5yr follow-up | 60,998 | Irregular sleep predicted 131 diseases; short sleep predicted 63 |
| Sleep consistency tied to activity and heart metrics | medRxiv (preprint) | Apple Heart and Movement Study, observational | 81,000+ (18M+ nights) | Most consistent tertile: +12 min/day exercise, −3.2 bpm resting HR |
| ML OSA screening via wearable phenotyping | Scientific Reports (Nature) | Prospective observational, ML dev/validation | 338 | AUC 0.94, F1 0.80 for OSA risk classification |
| Multi-night AI monitoring reduces OSA misdiagnosis | npj Digital Medicine (Nature) | Prospective clinical feasibility | 92 (3 months) | 92% feasibility; WSA 85% specificity, 77% sensitivity vs. single-night PSG |
| Psoriasis disrupts sleep via skin-to-brain TNF-α | Communications Biology (Nature) | Mouse model + clinical correlation | Mouse + clinical data | TNF-α inhibitor delivery to anterior hypothalamic area restored sleep |
| TASD prevalence in women | Communications Medicine (Nature) | Epidemiological cohort | 27,938 | 6.9% reported trauma-associated sleep disturbances in past month |
| Night-to-night variability modulates insomnia perception | Nature and Science of Sleep | Dense longitudinal EEG, MLM | 50 (312 nights) | N2 variability moderated the objective–subjective sleep discrepancy |
| DL identifies novel upper-face OSA markers | Nature and Science of Sleep | Cross-sectional DL + explainability | 130 | AUC 0.87; forehead/eyebrow region predicts OSA beyond mandibular features |
| 260 genes linked to sleep via rare coding variants | medRxiv (preprint) | Rare-variant GWAS meta-analysis | 600,000+ | 29 novel sleep-medication genes with distinct prenatal expression trajectories |
| Sleep quality gates MTL flexibility in older adults | medRxiv (preprint) | Cross-sectional fMRI + behavioral | 50 older adults | MTL flexibility predicted memory only in good sleepers (β=−1.519, p=.012) |
The regularity papers
The two most consequential publications this week did not come from a journal with peer review complete — both are medRxiv preprints, which means the findings should be treated as preliminary until peer review concludes. That caveat noted, the scale and design quality here are hard to set aside.
UK Biobank (Windred et al., Flinders University and Harvard): 60,998 participants, mean age 62.8, 10 million+ hours of objective sleep-wake data, 9.5 years of follow-up. 9 Irregular sleep was a stronger predictor than short sleep duration for 90 of 131 diseases analyzed — circulatory, metabolic, digestive, renal, neurological, musculoskeletal, and mental health disorders all showed stronger associations with variability than with duration. Short sleep duration outperformed irregularity for only 9 conditions. In 83% of the disease models where short sleep duration explained risk, adding sleep regularity further improved the predictive model.
Apple Heart and Movement Study (Komilian et al., Apple): 81,000+ participants, 18 million+ nights. 10 Across five different consistency metrics (total sleep time standard deviation, sleep start/end/midpoint SD, and Sleep Regularity Index), more consistent sleepers showed more physical activity, lower resting HR, and higher HRV. The most consistent tertile averaged 6.9 hours TST versus 5.9 hours in the least consistent — so they also slept longer. The authors note that causality cannot be established from this observational design.
These two datasets converge on the same directional conclusion from different populations, measurement methods, and outcome variables. The UK Biobank team (which includes researchers with disclosed ties to Withings and Oura, stated as unrelated to this work) used objective actigraphy over years; the Apple team used consumer smartwatch data. Neither alone would be definitive. Together, they are difficult to dismiss.
AI and ML in OSA screening
Two published papers this week tackled the core clinical bottleneck in sleep apnea: diagnosis requires an overnight lab study that most at-risk people never get.
Scientific Reports (Kim et al., Korea University): A multimodal ML model combining wearable sensors, smartphone usage metrics, and clinical scales (338 participants, 107 features, 4-week data collection) achieved AUC 0.94 for classifying high- versus low-risk OSA based on Berlin Questionnaire scores. 11 Top predictors were BMI, Insomnia Severity Index score, smartphone overuse score, resting heart rate, and heart rate recovery. The limitation worth noting: the study used the Berlin Questionnaire as the ground truth, not polysomnography. AUC 0.94 for predicting a questionnaire score is not the same as AUC 0.94 for detecting OSA against PSG.
npj Digital Medicine (Lechat et al., Flinders University): A prospective feasibility study (n=92, 53±15 years, 3-month monitoring) used the Withings Sleep Analyzer — an under-mattress device that estimates AHI without any worn hardware — to compare multi-night monitoring against single-night PSG. 12 92% of participants achieved ≥14 valid AHI nights in the first month. The device hit 85% specificity and 77% sensitivity versus PSG. More interesting: participants who had OSA detected by the under-mattress device but missed by PSG slept 97 fewer minutes during their lab night (p=0.027) and showed higher night-to-night AHI variability. Their PSG was clean partly because they slept badly in the lab — a known artifact. Multi-night home monitoring sidesteps that problem by averaging over many nights.
Also from this week: a deep learning model using frontal face photos and cephalograms (n=130, AUC 0.87) found that forehead, eyebrow, and upper eyelid geometry predicted OSA alongside traditional mandibular and hyoid features — a finding the authors describe as a novel phenotypic signal worth investigating for non-invasive screening. 13
A SLEEP 2026 clinical session on wearables for OSA diagnosis added context. Cathy Goldstein, MD (University of Michigan) reported that the Apple Watch's FDA-cleared OSA detection algorithm operates at 98.5% specificity and 66.3% sensitivity — intentionally tilted toward minimizing false positives. 14 The Samsung Galaxy Watch received FDA clearance for OSA risk monitoring in 2024. The session also surfaced a real-world access problem: wearable ownership is lower among adults ≥65, uninsured, rural, and Medicaid populations — the same groups who face diagnostic gaps.
Wearable research
Oura publishes three PPG algorithm validations
Oura's June 16 research blog post reported results from three PPG (photoplethysmography, the optical pulse-wave sensor in the ring) algorithm studies, validated against clinical reference standards. 15
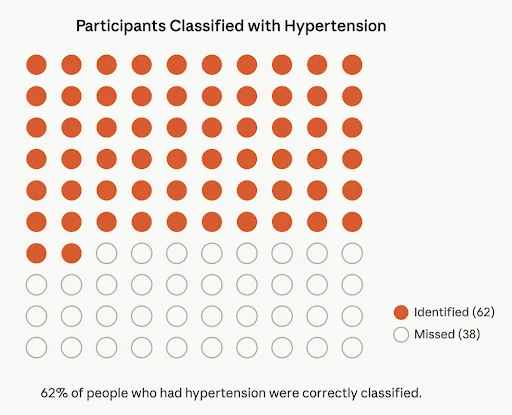
- Hypertension detection: Sensitivity 62%, specificity 91%, from the Blood Pressure Profile Study (300,000+ enrolled members).
- Nocturnal blood pressure dipping pattern: Sensitivity 84%, specificity 69%, AUC 0.87, validated against ambulatory blood pressure monitoring (ABPM) in 134 participants.
- Sleep apnea detection (eAHI): Sensitivity 76%, specificity 89% for moderate-to-severe OSA, validated against Type I PSG in 339 participants.
Oura's disclosure: the ring is a wellness product, not a medical device, and is not intended for diagnosis. The specificity figures — 91% for hypertension and 89% for OSA — mean that most people who screen negative are genuinely negative. The sensitivity figures mean the ring misses roughly 24–38% of true cases. That performance profile suits triage (flag people who might need follow-up) rather than diagnosis.
WHOOP and Weill Cornell: slow-wave sleep correlates with Alzheimer's cognition scores
WHOOP published results from a Weill Cornell Medicine (Cornell University) Alzheimer's prevention research collaboration on June 19. 16
The study enrolled 34 asymptomatic adults with family history of Alzheimer's disease, wearing WHOOP devices for six months. A machine-learning model classified participants into two groups based on WHOOP biometric data. The group with a higher percentage of slow-wave sleep scored higher on cognitive tests linked to prefrontal cortex function. Blood lipid and inflammation markers showed no group difference — the non-invasive wearable signal outperformed the invasive lab tests in correlating with cognitive performance.
The research team noted this is the first study to show wrist-worn wearable-identified slow-wave sleep associated with cognitive test performance. Sample size (n=34) limits the strength of any causal inference; the authors flag the need for larger replication. The underlying paper was published in the Journal of Prevention of Alzheimer's Disease.
Matthew Walker EP140: the physiology of "tired but wired"
Matthew Walker (UC Berkeley) published Episode 140 of The Matt Walker Podcast on June 15, titled "Tired but Wired." 17

The episode's core scientific claim: "Insomnia is often a disorder of hyperarousal rather than a lack of sleep drive." 17 The distinction matters because the standard lay model of insomnia — an empty fuel tank, not enough sleep pressure built up — points toward solutions like staying up later or sleeping in to accumulate debt. Hyperarousal points in the opposite direction: the system is idling high all day, not just at bedtime. Walker cites metabolic and brain-activity data showing the elevated state is a trait, not a nightly event.
正在加载内容卡片…
Walker reports that racing mind is cited ten times more often than racing body in people with insomnia. 18 The CBT-I toolkit he outlines for breaking the cycle:
- Cognitive shuffle: randomize your imagined mental images to prevent the brain from latching onto a coherent worry narrative
- Stimulus control: if you are lying awake, get out of bed — the bedroom should not be associated with wakefulness
- Rhythmic breathing: slow-paced breathing triggers a parasympathetic downshift, pulling the physiological throttle back
- Muscle relaxation: progressive relaxation addresses the somatic side of arousal that racing-mind framing can miss
The hyperarousal framing also explains why standard sleep hygiene advice often fails people with chronic insomnia: limiting caffeine or dimming lights addresses external inputs, but the internal throttle — a tonically elevated sympathetic state — remains untouched.
CBT-I and Alzheimer's cognition: a null result worth registering
Against the backdrop of optimism about sleep interventions and dementia risk, an RCT published June 16 in Alzheimer's & Dementia (Wiley) deserves attention. 19 200 cognitively normal older adults with insomnia symptoms were randomized to CBT-I (n=100) or control (n=100); outcomes were assessed at baseline, 6 weeks, and 1 year.
At 1 year, CBT-I did not improve information processing speed (mean difference 0.017, 95% CI −0.10 to 0.14, p=0.78), executive function (−0.09, p=0.40), or memory (0.41, p=0.77). Amyloid-beta deposition showed no group difference in a 50-person subsample. The authors' conclusion: "CBT-I did not improve cognitive performance or Aβ deposition by one year. Longer follow-up is needed to understand the potential impact of CBT-I on AD risk." 19 (NCT03954210)
One year may be too short a window to see amyloid changes or cognitive trajectory shifts; the study does not rule out longer-term effects. But the null at 1 year is a real data point, and anyone citing sleep intervention as a near-term cognitive booster in older adults should have this RCT in view.
Other findings from the week
Two additional papers from the Nature portfolio round out the picture. In a mouse model of psoriasis-like skin inflammation, Nanjing Medical University researchers found that sleep disruption — increased wakefulness and fragmented NREM — persisted even when itching was eliminated. 20 The pathway: skin-derived TNF-α elevated levels in the anterior hypothalamic area, driving overactivity of wake-promoting neurons. Delivering a TNF-α inhibitor directly to that brain region restored normal sleep in the mice — identifying a skin-to-brain axis as a potential therapeutic target for psoriasis-related insomnia that operates independently of itch.
A population study of 27,938 Icelandic women (SAGA cohort, ages 18–69) found that 6.9% reported trauma-associated sleep disturbances in the past month, with prevalence highest among young women and those with history of physical or sexual violence. 21 TASD was strongly associated with PTSD, depression, and anxiety — but the authors emphasize it as a distinct clinical signal that should be identified and addressed separately from those comorbidities, not subsumed under them.
A rare coding variant GWAS meta-analysis from Harvard's Broad Institute (n=600,000+, 36 sleep phenotypes) identified 260 genes associated with sleep. 22 The structurally interesting finding: self-reported sleep phenotype genes showed constant high prenatal expression, while sleep medication-use phenotype genes peaked in late prenatal development — suggesting that what we measure with questionnaires versus what drives sleep drug response may involve fundamentally different biological pathways.
This week's actionable insight: prioritize sleep consistency over sleep duration
Two independent preprints from datasets covering 142,000 people point in the same direction: irregular sleep is a worse disease predictor than short sleep. Going to bed and waking up at the same time every day — including weekends — is likely a higher-leverage variable than adding 30 minutes to your total sleep time, at least for long-term disease risk.
The one thing to test this week: track your social jet lag — the gap in minutes between your average weekday wake time and your weekend wake time. A gap of 90 minutes or more is associated with measurably worse health outcomes in the existing literature. If you use an Oura Ring or WHOOP, look at your sleep midpoint standard deviation across the past 14 nights (Oura shows this in the Trends view; WHOOP shows sleep start consistency). Bring that variability number below 30 minutes before you optimize sleep duration, supplement stacks, or wind-down protocols.
The SLEEP 2026 data adds a clinical dimension to this: COMISA — insomnia and sleep apnea together — does not just add risks, it multiplies them. If you regularly feel tired during the day and also have trouble falling asleep at night, those are not two separate problems. They may be a single combined phenotype that deserves clinical evaluation, not just a better mattress.
Cover image: Oura Ring research photo, used with Oura editorial permission.
参考来源
- 1Veterans with both insomnia and sleep apnea have elevated risk of developing type 2 diabetes
- 2Sleepy days and restless nights are a dangerous combination for blood pressure
- 3Women with sleep apnea report greater symptom burden than men
- 4Rural patients at high risk for obstructive sleep apnea are less likely to be referred for evaluation than urban patients
- 5Bedtime smartphone use linked to overnight phone activity in teens
- 6Oveporexton Phase 3 Results Show Benefits for Narcolepsy Type 1 Symptoms
- 7Jazz Pharmaceuticals Delivers Extensive Late-Breaking Data at SLEEP 2026
- 8Inspire Medical Systems announces presence at SLEEP 2026 and publication of PREDICTOR Study
- 9Sleep regularity outweighs sleep duration as a predictor of disease
- 10Consistency of sleep timing and duration are associated with more physical activity and favorable heart rate metrics
- 11Machine learning for scalable OSA risk screening using digital phenotyping
- 12Zero burden multi-night monitoring with AI enabled technology reduces OSA misdiagnosis
- 13Craniofacial features in OSA using explainable deep learning
- 14Wearables play pivotal role in diagnosing, identifying OSA
- 15What PPG can reveal: new cardiovascular and respiratory research findings
- 16Alzheimer's sleep data study finds slow wave sleep link
- 17The Matt Walker Podcast #140: Tired but Wired
- 18@sleepdiplomat on X: Why feel exhausted yet wide awake at 2 AM?
- 19The impact of CBT-I on cognitive performance and amyloid beta in older adults: an RCT
- 20A dermo-hypothalamic axis driven by TNF-α mediates sleep disturbances in psoriasis
- 21Trauma-associated sleep disturbances among women in a nationwide study
- 22Rare coding variants reveal distinct genetic architectures across sleep phenotypes
相似内容

Diet and Exercise Beat Metformin Over 20 Years — Plus: Fruit Juice, Fitness Trackers, and New Liver Transplant Guidelines
Chronic Disease Management Brief文章
3 New PubMed Papers: DASH Diet & BP, Isometric Exercise & Postbiotic Sleep
Daily PubMed Research Digest图文
Five papers: June 16, 2026
PubMed Top Medical Papers文章
围绕这条内容继续补充观点或上下文。