June 24, 2026 · 9:22 AM
GLP-1 as a Longevity Drug? The Aging-Clock Signal Is Real, but Narrow
A small post hoc analysis found semaglutide shifted several epigenetic aging clocks in adults with HIV-associated lipohypertrophy, but that is not proof of general anti-aging efficacy. This issue grades the GLP-1 longevity claim against human biomarkers, disease-endpoint trials, conflicts, and real geroscience progress.

Bottom line
Semaglutide has earned a serious longevity-science discussion, not a longevity-drug crown. The strongest new signal is human and randomized: a post hoc epigenetic-aging analysis of a 32-week phase 2b trial in adults with HIV-associated lipohypertrophy found slower movement on several DNA-methylation clocks, including DunedinPACE at 9% slower versus placebo. But the aging-clock endpoint was not pre-specified, the analyzed cohort was small, and the population was metabolically and immunologically specific. 1
This issue’s verdict: credible biomarker signal in a narrow human setting; no proof that GLP-1 drugs slow aging in healthy adults, extend lifespan, or should be used as anti-aging medicine. Nothing here is a dosing recommendation.
Hype Autopsy: the claim
Claim under autopsy: “GLP-1 drugs are becoming the first real longevity drugs.”
That claim did not come from nowhere. A 2025 Nature Biotechnology piece reported Novo Nordisk and Eli Lilly speakers telling an aging-research conference that GLP-1 receptor agonists may be the first longevity drugs, while also noting the crucial boundary: benefits for chronic diseases of aging are clear mainly in people with obesity, type 2 diabetes, or high baseline cardiometabolic risk; for “everyone else,” clinical data are lacking. 2
Now the semaglutide aging-clock paper gives the claim a sharper hook: “9% slower” biological aging. The hook is real. The leap is the problem.
Evidence ladder
| Claim | Evidence tier | Species / population | Study design | Effect size | What it can support |
|---|---|---|---|---|---|
| Semaglutide shifted several epigenetic aging clocks in this trial | Tier 5 — RCT-derived human biomarker evidence, qualified | Human; adults with HIV-associated lipohypertrophy | Post hoc exploratory analysis of a 32-week randomized, double-blind, placebo-controlled phase 2b trial; semaglutide n=45, placebo n=39 | PhenoAge −4.9 years/year; PCGrimAge −3.1; DunedinPACE −0.09 units, or 9% slower | A real short-term biomarker signal in a specific clinical population. 1 |
| Semaglutide reduces visceral fat in the parent HIV lipohypertrophy trial | Tier 5 — human RCT | Human; adults with HIV-associated lipohypertrophy without diabetes | Single-center, randomized, double-blind, placebo-controlled phase 2b trial; 108 randomized | Abdominal visceral adipose tissue −30.6% over 32 weeks; 8 withdrawals in each arm | Semaglutide can improve the trial’s actual target condition; it does not prove anti-aging efficacy. 3 |
| Wegovy reduces cardiovascular events in high-risk adults with obesity or overweight | Tier 5/6 for that disease endpoint, not for aging | Human; adults with established cardiovascular disease plus obesity or overweight | Multinational, placebo-controlled, double-blind trial with over 17,600 participants | Major adverse cardiovascular events: 6.5% with Wegovy vs 8% with placebo | Hard clinical benefit in a high-risk disease population; not an “aging” indication. 4 |
| GLP-1 drugs slow aging in healthy adults or extend lifespan | Tier 1 — mechanistic plausibility, not demonstrated | Human general population: not tested | No published healthy-adult longevity trial establishing this claim | No lifespan, healthspan-composite, or replicated clinical-aging endpoint | A marketing claim, not a clinical conclusion. 2 |
What the semaglutide paper actually showed
The new Nature Communications study is best read as a biomarker add-on to an existing clinical trial, not as a standalone anti-aging trial. The parent trial asked whether semaglutide reduces abnormal visceral fat accumulation in people with HIV-associated lipohypertrophy. The aging-clock analysis was added afterward. 1 3
| Design question | Answer |
|---|---|
| Randomized? | Yes, in the parent trial: semaglutide vs placebo. 3 |
| Pre-specified aging endpoint? | No. The paper states epigenetic aging was not pre-specified. 1 |
| Sample for clock analysis | 84 people: semaglutide n=45, placebo n=39. 1 |
| Duration | 32 weeks. 1 |
| Strongest headline number | DunedinPACE −0.09 units, described as 9% slower; p=0.01. 1 |
| Main limitation | Post hoc design, modest sample size, HIV-specific cohort, short follow-up, peripheral-blood clocks rather than clinical aging outcomes. 1 |
The parent trial strengthens the biology but narrows the conclusion. Semaglutide reduced visceral adipose tissue by about 30.6% and total body fat by about 18.9% over 32 weeks in the HIV lipohypertrophy trial; it also produced one semaglutide-related grade 4 elevated lipase case and two possibly related cholelithiasis cases. 3 That is a credible metabolic intervention signal in a medically specific group. It is not evidence that metabolically healthy people should pursue GLP-1 therapy for longevity.
Why GLP-1s are tempting to the longevity field
The best case for GLP-1s is not “mice lived longer” or influencer biohacking. It is that these drugs already have human disease-endpoint data in conditions that rise with age.
Wegovy’s cardiovascular indication is the cleanest example: the FDA approved semaglutide injection to reduce cardiovascular death, heart attack, and stroke risk in adults with established cardiovascular disease plus obesity or overweight; in the cited trial, major adverse cardiovascular events occurred in 6.5% of Wegovy-treated participants versus 8% on placebo. 4 That is real medicine. It also explains why aging researchers are interested: inflammation, visceral adiposity, liver fat, vascular risk, kidney disease, and neurodegeneration all sit near aging biology. 2
The boundary is equally important: reducing disease events in high-risk patients is not the same as slowing organismal aging. A drug can be excellent for obesity-related cardiometabolic risk and still fail as a general gerotherapeutic.
Diffusion Tracker: how the claim travels
- Specialist conference framing: GLP-1s are discussed by major drugmakers in the language of longevity and preventive medicine. 2
- Biomarker headline: A randomized-trial-derived analysis reports “9% slower” DunedinPACE in a small HIV lipohypertrophy cohort. 1
- Institutional press translation: UC San Diego framed the result as a popular GLP-1 drug that “may slow down biological aging,” while quoting the lead author saying they are not claiming semaglutide reverses aging or makes people younger. 5
- Consumer-risk zone: “May influence aging biology” becomes “anti-aging drug” once the caveats fall away: HIV cohort, post hoc endpoint, 32 weeks, clocks rather than disease-free survival.
Follow the Money
This claim travels through a huge commercial market. Novo Nordisk reported 2025 sales of DKK 309.064 billion; obesity-care sales reached DKK 82.347 billion, GLP-1-based type 2 diabetes products reached DKK 152.202 billion, and Ozempic alone reached DKK 127.089 billion. 6 The same report says sales and distribution costs were driven partly by promotional activities related to Wegovy and international Wegovy launches. 6
The semaglutide epigenetic-aging paper itself was NIH-supported, not company-sponsored, which matters. Its conflict layer still matters: one author is a scientific advisor for TruDiagnostic, and two authors are TruDiagnostic employees; another serves as a research consultant for Merck, GSK/ViiV, and Gilead. 1 That does not invalidate the result. It means readers should separate assay-company incentives, drug-company market incentives, and the actual statistical signal.
Real Progress Watch
The useful progress this week is not “Ozempic is anti-aging now.” It is that aging measurement is becoming testable enough to disappoint hype.
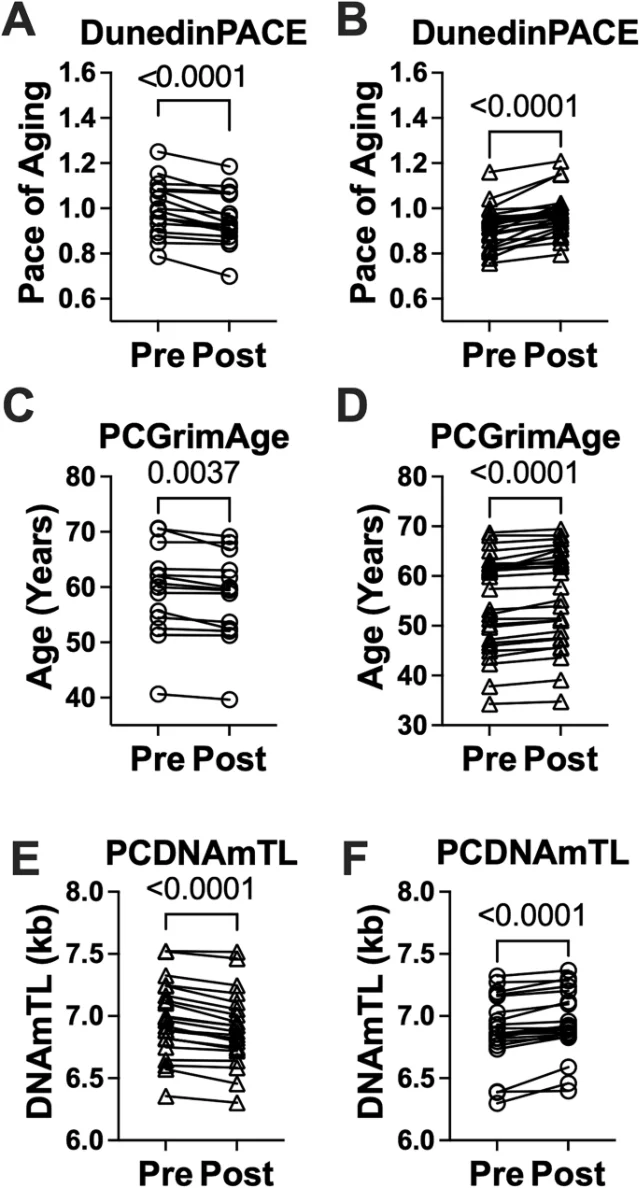
First, the GLP-1 biomarker story is not uniformly positive. In the 24-week SLIM LIVER single-arm semaglutide pilot in 41 people with HIV and MASLD, the overall group did not show a clean clock-wide “younger” pattern: DunedinPACE changed by a median +0.018, PCGrimAge by +0.54 years, and PCDNAmTL by −0.006 kb. Subgroups with improved DunedinPACE had greater liver-fat reduction, but the authors explicitly call the analysis exploratory and uncontrolled. 7
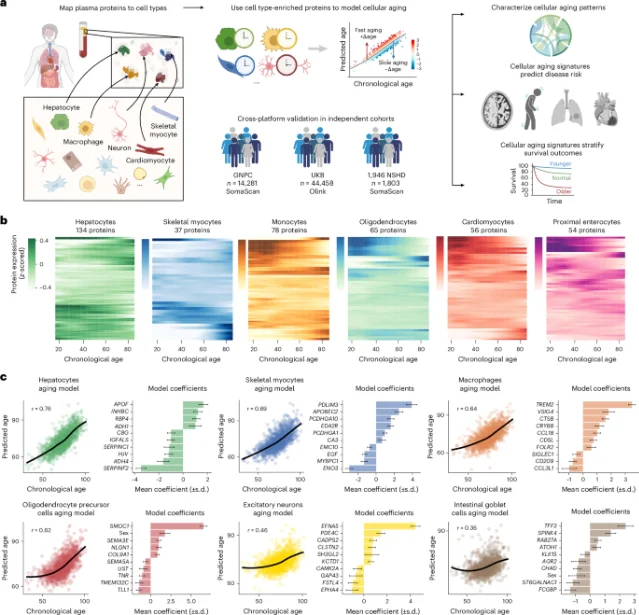
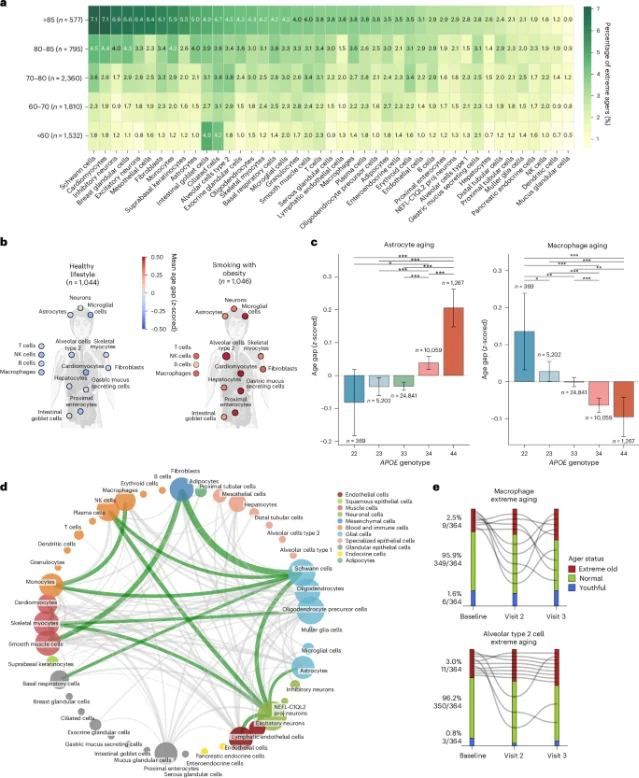
Second, a separate Nature Medicine study shows what a stronger aging-biomarker field is trying to become: 60,542 people, more than 7,000 plasma proteins, models for over 40 cell types, and 15-year disease and mortality follow-up. It linked cell-type-specific aging patterns with future disease risk, including skeletal myocyte aging with ALS risk and respiratory epithelial aging plus smoking with higher lung-cancer risk. 8
That is not a drug proof either. It is progress toward biomarkers that can be judged against real outcomes.
Reader checklist: when a longevity claim uses an aging clock
Before accepting the claim, ask five questions:
- Whose aging? Healthy adults, older adults, people with obesity, diabetes, HIV, MASLD, or another high-risk condition?
- Which endpoint was planned? Pre-specified clinical endpoint, pre-specified biomarker, or post hoc exploration?
- What changed besides the clock? Disease events, physical function, organ fat, inflammation, mortality risk, or just molecular score movement?
- How long? Weeks and months can detect biomarker movement; they cannot establish durable healthspan benefit.
- Who benefits if the weak version becomes the public version? Drugmaker, supplement seller, testing company, clinic, influencer, or patient?
Verdict table
| Claim | Verdict | Why |
|---|---|---|
| “Semaglutide affected aging-related biomarkers in a randomized human trial.” | Plausible and worth following. | Human RCT-derived data, multiple clocks, but post hoc and small. 1 |
| “GLP-1s are promising geroscience candidates.” | Reasonable hypothesis. | Strong metabolic and cardiovascular human data in high-risk populations; plausible inflammation and organ-risk biology. 2 4 |
| “Semaglutide is proven to slow aging in ordinary healthy adults.” | Not shown. | No published healthy-adult longevity trial, no replicated healthspan endpoint, no lifespan evidence. 2 |
| “Aging clocks are useless because this is not definitive.” | Wrong direction. | Biomarkers are useful when they are treated as instruments to test, not as proof substitutes. The better the clock, the more falsifiable the claim. 8 |
Final grade: GLP-1 longevity claim = Tier 5 for a narrow biomarker effect in one small randomized human setting; Tier 1 for general-population anti-aging. The correct sentence is not “semaglutide is a longevity drug.” It is: “semaglutide has a serious, early human aging-biomarker signal that now needs prospective, longer, independently replicated trials with clinical outcomes.”
References
- 1Nature Communications — semaglutide epigenetic aging trial
- 2Nature Biotechnology — Are GLP-1s the first longevity drugs?
- 3PMC — parent Lancet Diabetes & Endocrinology trial
- 4FDA — Wegovy cardiovascular-risk indication
- 5UC San Diego Today — GLP-1 drug may slow biological aging
- 6Novo Nordisk Annual Report 2025 — financial performance
- 7npj Aging — SLIM LIVER semaglutide epigenetic-aging pilot
- 8Nature Medicine — plasma proteomic signatures of cellular aging



Add more perspectives or context around this Post.