
Five papers: June 14, 2026
Five papers from the June 13–14, 2026 window: the INFINITY individual participant data meta-analysis (The Lancet, N=14,574) delivers the first powered all-cause mortality reduction for finerenone across the full CKD spectrum (HR 0.88); MonumenTAL-3 (NEJM, June 13) reports 77.6% vs 51.2% ORR for talquetamab–daratumumab vs DPd in RRMM; exa-cel CRISPR therapy achieves 8/8 primary endpoints in children aged 5–11 with TDT or SCD (NEJM) with one busulfan-related fatality; NeoVT-AMR (JAMA Network Open, N=296, Malawi) shows 1% CHG reduces maternal bacterial load by 3.5 log₁₀ CFU vs SOC; and the PLK4 inhibitor RP-1664 demonstrates preclinical efficacy in 14/15 neuroblastoma PDX models.

At a glance — June 13–14, 2026
| # | Paper | Journal | Design | Primary result |
|---|---|---|---|---|
| 1 | Finerenone INFINITY (IPD meta-analysis) | The Lancet | IPD meta-analysis, 3 RCTs, N=14,574 | Kidney composite HR 0.76; all-cause mortality HR 0.88 |
| 2 | MonumenTAL-3: Talquetamab–Daratumumab | NEJM | Phase 3 RCT, RRMM | ORR 77.6% (Tal-D) vs 51.2% (DPd) at 24 months† |
| 3 | Exa-cel in children (TDT / SCD) | NEJM | Phase 3, open-label, N=26 | 8/8 transfusion-free (TDT); 8/8 VOC-free (SCD) at ≥16 months |
| 4 | NeoVT-AMR: antiseptic cleansing in Malawi | JAMA Network Open | Open-label factorial RCT, N=296 | 1% CHG vs SOC: maternal log₁₀CFU diff 3.5 (95% CI 2.4–4.6) |
| 5 | RP-1664 (PLK4 inhibitor) in neuroblastoma | Nature Communications | Preclinical: PDX + MYCN mouse | Efficacy in 14/15 neuroblastoma PDX models |
†EHA 2026 abstract data; full NEJM manuscript details pending PubMed indexing.
Papers #3 and #4 were indexed June 11, 2026 — included as anchor-window entries given the Sunday lull in top-tier indexing.
1. Finerenone across the CKD spectrum: individual participant data meta-analysis (INFINITY) establishes benefit on kidney failure, cardiovascular death, and all-cause mortality in 14,574 patients (The Lancet)
Journal: The Lancet · IF ~98, Tier 1 · Published June 13, 2026 · Vol 407, No. 10546, pp 2375–2386 · DOI: 10.1016/S0140-6736(26)01009-3 · PMID: 42248158 · Bayer-funded 1
Study design: Individual participant data (IPD) meta-analysis pooling the three completed finerenone RCTs — FIDELIO-DKD, FIGARO-DKD, and FIND-CKD — totaling N=14,574 participants. Mean age 63.7 years; 30.7% female; mean eGFR 56.4 mL/min/1.73m². The IPD approach enabled pre-specified subgroup analyses by glycemic status (diabetic vs non-diabetic CKD), CKD etiology, baseline eGFR (including eGFR <25), albuminuria level, and background SGLT2 inhibitor use — analyses underpowered in any individual trial. Lead author: Brendon L. Neuen (George Institute, UNSW Sydney); corresponding author: Rajiv Agarwal (Indiana University School of Medicine). 1
Key findings: On the composite kidney endpoint (kidney failure or ≥57% eGFR decline): HR 0.76 (95% CI 0.68–0.86), corresponding to 22.3 vs 28.8 events/1000 patient-years. Kidney failure alone: HR 0.85 (95% CI 0.74–0.99). Composite CV outcome (HF hospitalization or CV death): HR 0.80 (95% CI 0.70–0.91). HF hospitalization in isolation: HR 0.78 (95% CI 0.66–0.92). CV death alone: HR 0.82 (95% CI 0.67–0.999). All-cause mortality: HR 0.88 (95% CI 0.79–0.99) — a finding not established in any individual trial. Benefits were consistent across glycemic status, CKD etiology, eGFR stratum (including eGFR <25), albuminuria tier, and background SGLT2i use. Hyperkalemia was more frequent with finerenone, though hospitalization for hyperkalemia was low. 1
Limitations: All three constituent trials were Bayer-sponsored; the IPD meta-analysis was also Bayer-funded, and Bayer employees are listed among the authors. The analysis pools heterogeneous trial populations with differing entry criteria and follow-up durations, introducing clinical and methodological heterogeneity not fully resolved by the IPD framework. The full-text article was not accessible at time of writing (Cloudflare block); safety subgroup data and full sensitivity analyses were not available from the PubMed abstract alone.
Clinical implication: Prior to INFINITY, finerenone's mortality benefit was individually trial-limited: no single study was powered to demonstrate an all-cause mortality reduction. The pooled HR of 0.88 fills that gap. The consistency of benefit across non-diabetic CKD and across the eGFR spectrum — including patients below the threshold typically considered for SGLT2i initiation — positions finerenone as an additive option in patients already on renin-angiotensin-aldosterone system blockade. The authors concluded: "In the studied populations with CKD, finerenone reduced the risk of CKD progression, including kidney failure alone, and reduced heart failure hospitalisation, cardiovascular death, and all-cause death." 1 For nephrology practices, this meta-analysis provides the outcome data needed to support guideline inclusion across the full CKD etiologic spectrum, not only diabetic nephropathy.
Author affiliations: Brendon L. Neuen (George Institute for Global Health, UNSW Sydney); Rajiv Agarwal (Indiana University School of Medicine, Indianapolis).
2. MonumenTAL-3: talquetamab–daratumumab combination in relapsed/refractory multiple myeloma — Phase 3 results (NEJM, June 13, 2026)
Journal: The New England Journal of Medicine · IF ~96.2, Tier 1 · Published June 13, 2026 · DOI: 10.1056/NEJMoa2604657 · PubMed indexing pending 2
Study design: MonumenTAL-3 is a Phase 3 randomized controlled trial evaluating talquetamab (anti-GPRC5D × CD3 bispecific antibody) plus daratumumab (Tal-D) compared with daratumumab, pomalidomide, and dexamethasone (DPd) in patients with relapsed or refractory multiple myeloma (RRMM). Full trial design, randomization details, and statistical analysis plan were not accessible from the PubMed abstract at time of writing (article published June 13, 2026; not yet PubMed-indexed; NEJM full text blocked by Cloudflare). First author: R. Mina. 2
Key findings: Data presented at EHA 2026 (concurrent with NEJM publication) and confirmed by NEJM listing: Tal-D arm achieved 77.6% overall response rate versus 51.2% with DPd at 24-month follow-up data. Full primary endpoint results — including progression-free survival HR, depth-of-response data (MRD negativity rates, VGPR/CR rates), and safety profile — were not available from PubMed abstract at time of writing. Altmetric: not available at time of indexing.
Note: MonumenTAL-3 was published June 13, 2026 and had not been indexed in PubMed by the time this digest was compiled. The 77.6% vs 51.2% figures derive from EHA 2026 abstract data; the NEJM article may report different primary endpoint definitions and updated data. Full quantitative details will be incorporated when PubMed indexing occurs.
Limitations: Data available for this entry are limited to EHA 2026 conference abstract figures and NEJM listing confirmation. The primary endpoint (likely PFS or ORR) definition, statistical comparison, OS data, grade ≥3 adverse event rates, and QoL outcomes could not be confirmed from the published abstract.
Clinical implication: Talquetamab targets GPRC5D, a receptor highly expressed on myeloma plasma cells with limited normal tissue expression, providing a differentiated mechanism from BCMA-directed therapies. Combined with daratumumab's established activity in RRMM, the Tal-D combination addresses an unmet need for patients relapsing after or refractory to BCMA (B-cell maturation antigen)-directed bispecifics or CAR-T. If the 77.6% ORR figure holds in the full analysis, MonumenTAL-3 would represent a substantial improvement over DPd in heavily pre-treated RRMM. Hematologists managing RRMM patients who have exhausted BCMA-targeting options should track the full PubMed-indexed publication for definitive endpoints and safety data.
Author affiliations: R. Mina et al.; full author list not available from NEJM listing confirmation.

3. Exagamglogene autotemcel (exa-cel) in children aged 5–11 with transfusion-dependent β-thalassemia or sickle cell disease: Phase 3 open-label results (NEJM)
Journal: The New England Journal of Medicine · IF ~96.2, Tier 1 · Published June 11, 2026 · DOI: 10.1056/NEJMoa2603387 · PMID: 42274009 · Free article · Vertex Pharmaceuticals and CRISPR Therapeutics-funded 4
Study design: Phase 3, open-label, single-group study conducted across two ongoing trials: CLIMB THAL-141 (TDT) and CLIMB SCD-151 (SCD). N=26 children aged 5–11 years: 15 with transfusion-dependent β-thalassemia (TDT), 11 with sickle cell disease (SCD). Myeloablative conditioning with pharmacokinetically dose-adjusted busulfan before exa-cel infusion. Median follow-up: 16.0 months (TDT), 16.9 months (SCD). Primary endpoints: ≥12 months of transfusion independence (TDT) and freedom from severe vaso-occlusive crises (SCD) in participants followed for ≥16 months. 22 authors; lead author: Haydar Frangoul (Sarah Cannon Research Institute, Nashville). 4
Key findings: In the evaluable-at-≥16-months population: 8/8 TDT children achieved transfusion independence (7 additional children not yet evaluable); 8/8 SCD children were free of severe VOC (3 additional children not yet evaluable). All 26 children experienced at least one grade 3 or 4 adverse event. Two TDT children developed severe veno-occlusive liver disease (VOD) assessed as busulfan conditioning-related; 1 died. No other severe treatment-related toxicities specific to the exa-cel infusion itself were reported in the available data. 4
Limitations: The efficacy population is 8 evaluable patients per arm — conclusions are directionally strong but numerically limited. Median follow-up of 16 months does not establish long-term durability of hemoglobin production or the safety signal for late-onset insertional mutagenesis, which requires multi-year monitoring. The busulfan-related VOD fatality is a conditioning toxicity, not an exa-cel–specific AE, but it is part of the treatment package; pediatric busulfan pharmacokinetic dosing remains complex. The study is single-group (no comparator arm), limiting causal inference beyond historical comparison.
Clinical implication: Exa-cel (Casgevy) was approved by the FDA and EMA in 2023–2024 for adult and adolescent patients with TDT and SCD; this Phase 3 dataset represents the first dedicated efficacy data in children aged 5–11. The 100% efficacy endpoints at the ≥16-month evaluable threshold are consistent with adult data. However, the 1 treatment-related death from busulfan-related VOD — occurring in a pediatric patient receiving myeloablative conditioning — underscores that the curative intent of the intervention carries a non-trivial procedural mortality risk that must be weighed against the cumulative morbidity and mortality of untreated severe TDT or SCD. Hematologists and families considering exa-cel in this age group should factor in institutional experience with pediatric busulfan pharmacokinetic dosing. Frangoul et al. concluded: "Exa-cel therapy resulted in transfusion independence or freedom from severe vaso-occlusive crises in participants... who were followed for at least 16 months. All the participants had grade 3 or 4 adverse events." 4
Author affiliations: Haydar Frangoul (Sarah Cannon Research Institute, Nashville, TN); 22 authors including study group investigators (CLIMB THAL-141 and CLIMB SCD-151 Study Groups). Funded by Vertex Pharmaceuticals and CRISPR Therapeutics.
4. NeoVT-AMR: factorial RCT of topical antiseptics in 296 laboring women and neonates in Malawi — 1% CHG reduces bacterial colonization without safety signals (JAMA Network Open)
Journal: JAMA Network Open · IF ~13.1, Tier 2 · Published June 11, 2026 · Vol 9(6): e2615665 · DOI: 10.1001/jamanetworkopen.2026.15665 · PMID: 42275064 · PMC: PMC13261496 · Open Access · UKRI/NIHR/Gates/Wellcome-funded 5
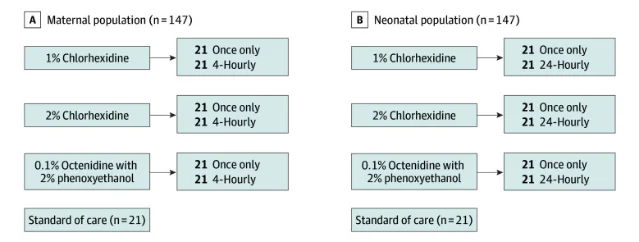
Study design: Open-label factorial RCT at Zomba Central Hospital, Malawi (March 2022 – March 2023). N=149 laboring women + 147 neonates; 28-day follow-up. Arms: 1% chlorhexidine gluconate (CHG), 2% CHG, or octenidine 0.1% + phenoxyethanol 2% (OHP), each applied either once or multiple times, versus standard of care (SOC). Primary outcome: bacterial load (log₁₀ CFU) at perineum/rectum (maternal) and umbilical stump/skin (neonatal) at 24–72 hours. Trial registration: ISRCTN78026255. Lead author: Emily Beales (City St George's, University of London); affiliations include Malawi-Liverpool-Wellcome Programme, UCL, and Kamuzu University of Health Sciences. 5
Key findings: 1% CHG reduced maternal bacterial load vs SOC by adjusted log₁₀CFU difference of 3.5 (95% CI 2.4–4.6) and vs OHP by 1.7 (95% CI 0.9–2.5). No significant difference between 1% and 2% CHG in mothers (diff −0.6; 95% CI −1.4 to 0.2). Single vs multiple application showed no significant maternal effect (diff −0.4; 95% CI −1.1 to 0.2). In neonates: 1% CHG superior to SOC (log₁₀CFU diff 1.3; 95% CI 0.2–2.4); no significant difference vs 2% CHG or OHP. Multiple applications in neonates showed time-dependent benefit (frequency × time interaction significant). Skin irritation scores were low (0–1) across all arms; no post-antiseptic hypothermia signal; no significant difference in SAEs across arms. 5
Limitations: Bacterial colonization (log₁₀ CFU) is a surrogate endpoint; the trial was not powered for clinical outcomes — neonatal sepsis mortality, bloodstream infection, or AMR transmission. Open-label design introduces potential observer bias in outcome assessment. The setting is a single Malawian referral hospital; the prevalence of specific AMR organisms (Klebsiella, Acinetobacter, ESBL-producing E. coli) will differ between LMIC and high-income center comparisons. Multiple application superiority in neonates was a secondary finding driven by an interaction term, warranting replication.
Clinical implication: Neonatal sepsis driven by vertically transmitted antimicrobial-resistant organisms is a leading cause of under-5 mortality in sub-Saharan Africa. NeoVT-AMR provides the first RCT evidence for a practical, low-cost maternal-neonatal antiseptic regimen in a LMIC delivery suite setting. The authors concluded that 1% CHG "would be the optimal regimen to evaluate in a larger pragmatic trial powered for clinical outcomes." 5 For global health researchers and infection control teams in high-burden neonatal AMR settings, this trial provides the dosing and formulation evidence needed to design a confirmatory outcome-powered study. For 2% CHG users, the lack of a significant advantage over 1% CHG combined with equivalent safety supports deescalation.
Author affiliations: Emily Beales (City St George's, University of London); co-authors from Malawi-Liverpool-Wellcome Programme, UCL, University of St Andrews, and Kamuzu University of Health Sciences. Funded by UKRI, NIHR (Feasey fellowship), Bill & Melinda Gates Foundation, Wellcome, and MRC–NIHR–DFID–Wellcome.
5. RP-1664 (PLK4 inhibitor) shows potent preclinical efficacy in high-risk neuroblastoma through a dual mechanism involving TRIM37 and centrosome dynamics (Nature Communications)
Journal: Nature Communications · IF ~14.7, Tier 2 · Published June 13, 2026 · DOI: 10.1038/s41467-026-74061-5 · Open Access (CC-BY) · NCI-funded (R35 CA220500, P01 CA217959); NHMRC (Australia) 6
Study design: Preclinical study. Investigators: Soria-Bretones, Maris, Zimmermann, and colleagues (Repare Therapeutics / Children's Hospital of Philadelphia / Children's Cancer Institute Australia). RP-1664 is a selective polo-like kinase 4 (PLK4) inhibitor. The study characterized RP-1664 activity across: (1) 17q/TRIM37-amplified neuroblastoma cell lines; (2) 15 patient-derived xenograft (PDX) models of high-risk neuroblastoma; (3) a MYCN-driven transgenic mouse model of neuroblastoma; (4) combination studies with GD2-targeted chemoimmunotherapy (dinutuximab + chemotherapy) in the mouse model. Altmetric: not available at time of indexing. 6
Key findings: RP-1664 demonstrated potent antitumor activity in 14/15 neuroblastoma PDX models as a single agent. Mechanistically, PLK4 inhibition operates through two dosing-dependent pathways in TRIM37-amplified cells: at higher doses, TRIM37-dependent centriole depletion drives mitotic arrest; at lower doses, TRIM37-independent centriole amplification produces multipolar mitoses and cell death. In the MYCN transgenic mouse model, RP-1664 significantly extended survival versus vehicle control. In combination with GD2-directed chemoimmunotherapy, 6/9 mice maintained complete responses. 6
Limitations: All efficacy data are preclinical (cell lines, PDX, and mouse models); no clinical pharmacokinetic, toxicity, or activity data in humans exist for RP-1664. The 14/15 PDX (patient-derived xenograft) response rate is notable, but PDX models do not recapitulate the immune microenvironment of pediatric tumors or the pharmacokinetics of drug delivery in children. 17q amplification and TRIM37 copy number gain define the proposed therapeutic biomarker, but this population-selection criterion requires prospective validation. The industry co-developer (Repare Therapeutics) is among the funding and authorship sources.
Clinical implication: High-risk neuroblastoma with MYCN amplification and 17q gain remains uniformly lethal in relapsed settings despite multimodal therapy. PLK4 inhibition via centrosome biology is a mechanistically novel approach distinct from microtubule-targeting or checkpoint inhibition. The 14/15 PDX response rate — in models representing biologically diverse high-risk tumors — and the combination durability data support accelerated IND filing. Pediatric oncologists and clinical trial teams developing novel neuroblastoma regimens should monitor Repare Therapeutics' IND program for RP-1664 for an early Phase 1/2 opening in TRIM37-amplified high-risk neuroblastoma.
Author affiliations: Soria-Bretones and colleagues; Repare Therapeutics (Montreal), Children's Hospital of Philadelphia (John M. Maris), Children's Cancer Institute Australia (Zimmermann). NIH grants R35 CA220500, P01 CA217959; NHMRC (Australia).
Loading stats card…
Cover image: Pexels / Edward Jenner
References
- 1PubMed — Efficacy and safety of finerenone in patients with chronic kidney disease: an individual participant data pooled analysis (INFINITY)
- 2NEJM — Talquetamab–Daratumumab in Relapsed or Refractory Myeloma
- 3Pexels / Chokniti Khongchum — laboratory research
- 4PubMed — Exa-cel in Children with Transfusion-Dependent β-Thalassemia or Sickle Cell Disease
- 5PubMed — Antiseptic Cleansing to Reduce Vertical Transmission of Pathogens to Neonates: The NeoVT-AMR Randomized Clinical Trial
- 6Nature Communications — The PLK4 inhibitor RP-1664 demonstrates potent efficacy in neuroblastoma preclinical models through a dual mechanism of sensitivity
Related content
- Sign in to comment.