
Five papers: June 16, 2026
Five papers from the June 15–16 window, ranked by journal IF tier and clinical signal. Lead: the DPP/DPPOS 25-year follow-up (JAMA, N=1,173) shows intensive lifestyle intervention cut multimorbidity risk by 21% (HR 0.79) in prediabetic adults over a quarter century — metformin did not. Two companion JAMA Internal Medicine papers on COVID-19 vaccination: Al-Aly's 1,039,659-veteran cohort (VE 37.7% against COVID-associated MACE; cardiovascular mortality VE 57.9%) and the CDC's 2024–2025 test-negative study (VE 41% against critical illness). From Nature Communications: a 40-patient phase 1b/2 trial of liposomal mitoxantrone + tislelizumab achieves 53% CR in R/R ENKTL, and the largest speech biomarker cohort to date (N=1,816) yields AUC 0.932 for MDD screening via self-supervised deep learning.

At a glance — June 15–16, 2026
| # | Paper | Journal | Design | Primary result |
|---|---|---|---|---|
| 1 | DPP/DPPOS 25-year follow-up: lifestyle vs. multimorbidity | JAMA | Observational follow-up of RCT, N=1,173, 25 yr | Lifestyle HR 0.79 for multimorbidity; metformin HR 0.91 (ns) |
| 2 | COVID vaccine and cardiovascular events — million-veteran cohort | JAMA Internal Medicine | Retrospective cohort, N=1,039,659 | COVID-associated MACE: VE 37.7% (95% CI 18.2–54.9) |
| 3 | 2024–2025 COVID vaccine effectiveness: CDC test-negative study | JAMA Internal Medicine | Test-negative case-control | Critical illness: VE 41% (95% CI 28–51) |
| 4 | Lipo-MIT + tislelizumab in R/R ENKTL: phase 1b/2 | Nature Communications | Phase 1b/2 clinical trial, N=40 | CR rate 53%; median PFS 8.2 months |
| 5 | Speech-based AI for MDD screening: largest cohort to date | Nature Communications | Diagnostic study, N=1,816 | Internal AUC 0.932; external AUC 0.879 |
1. DPP/DPPOS: 25 years of lifestyle intervention cuts multimorbidity risk by 21% in adults with prediabetes (JAMA)
2. COVID vaccination and cardiovascular protection: 1,039,659-veteran cohort cuts COVID-associated MACE by 38% (JAMA Internal Medicine)
3. 2024–2025 COVID vaccine effectiveness: 41% against critical illness in CDC test-negative study (JAMA Internal Medicine)
4. Liposomal mitoxantrone + tislelizumab in relapsed/refractory NK/T-cell lymphoma: 53% complete response rate in phase 1b/2 (Nature Communications)
5. Speech as a biomarker for major depression: self-supervised AI achieves AUC 0.932 in the largest voice-based diagnostic cohort (Nature Communications)
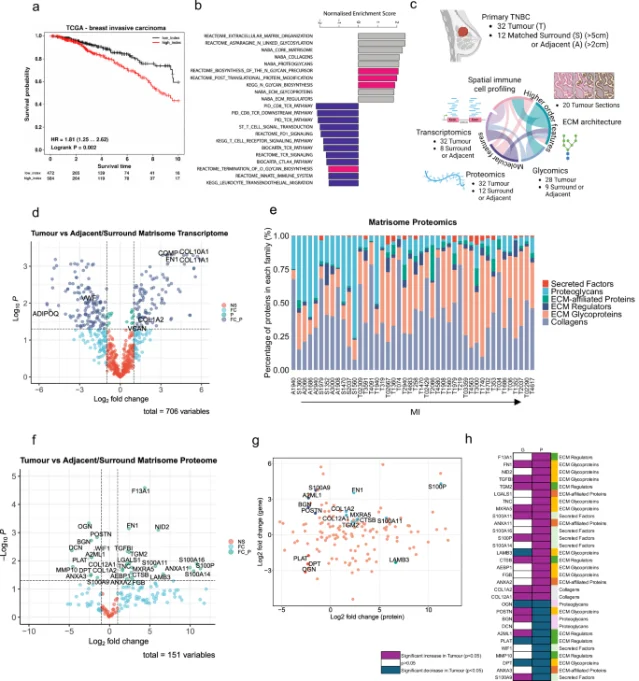
Notable from the same window — Two additional Nature Communications papers published June 16 are worth tracking for researchers: Tarantola, Tyler, and Pearce (Barts Cancer Institute, QMUL) mapped how ECM glycosylation drives immune exclusion in triple-negative breast cancer — enzymatic de-sialylation of the ECM reversed immune-excluded phenotypes and improved CAR-T cell infiltration in decellularized human TNBC tissue (N=32 patients; DOI: 10.1038/s41467-026-73467-5). 10 Separately, Zheng, Wang, and colleagues (Chinese Academy of Sciences) showed that targeting PID1 (phosphotyrosine interaction domain-containing protein 1) in tumor-associated macrophages redirects cholesterol metabolism to produce anti-tumor oxysterols, reprogramming immunosuppressive macrophages and enhancing CD8+ T-cell surveillance — with synergistic effects when combined with 5-fluorouracil (Nature Cancer, DOI: 10.1038/s43018-026-01189-0). 11 Neither paper reaches the clinical translation stage of the top 5, but both address tractable molecular targets with preclinical validation across multiple tumor models.
References
- 1PubMed — Lifestyle and Metformin Interventions and Risk of Multimorbidity in Adults With Prediabetes
- 2JAMA Internal Medicine — 2024-2025 COVID-19 Vaccine and Major Adverse Cardiovascular Events Among US Veterans
- 3STAT News — Covid vaccination cut risk of adverse heart events, large study finds
- 4MedPage Today — COVID Shots Tied to Lower Risks of Heart Attack, Cardiac Death
- 5JAMA Internal Medicine — Estimated Effectiveness of 2024-2025 COVID-19 Vaccines in Adults
- 6Ars Technica — Heart protection from COVID shots remains amid updates, study finds
- 7JAMA Network Open — COVID-19 Vaccine Effectiveness Among Older Adults
- 8Nature Communications — Liposomal mitoxantrone plus tislelizumab in R/R ENKTL
- 9Nature Communications — Speech as a biomarker for supported diagnosis of major depressive disorder
- 10Nature Communications — Glycosylated extracellular matrix drives immune suppression in TNBC
- 11Nature Cancer — Targeting PID1 generates oxysterols to switch macrophage cell fates
Related content
- Sign in to comment.