
www.nature.com
Inside REM sleep's hidden gatekeeper
Week of May 24–31, 2026: a Nature Neuroscience paper from the Weber lab (U Penn) reveals two brainstem principal components that predict NREM→REM transitions 110 seconds in advance — a mechanistic explanation for why alcohol, sedatives, and late bedtimes fragment REM. Two large wearable datasets (WHOOP's 1.2-million-day menstrual cycle study; Harvard's 94,118-night Apple Watch perimenopause study) converge on women's sleep deterioration beyond aging. Plus: OSA spindle recovery, a Bayesian walking meta-analysis (g=−0.76), CBT for menopausal insomnia, Oura Ring 5 launch, WHOOP jet lag review, and Matt Walker's Nightfall IQ clinical platform. Actionable insight: 30-minute moderate walks, 4×/week for 12 weeks.
Your brain decides to enter REM sleep about 110 seconds before it actually happens — and a new Nature Neuroscience paper published this week shows exactly what is doing the deciding. That finding leads a week in which wearable datasets at extraordinary scale (1.2 million device-days, 94,000 tracked nights) converge with bench neuroscience to close two long-standing gaps: why REM is so fragile, and why women's sleep deteriorates faster than aging alone explains.
This week in sleep research
1. A brainstem circuit predicts your next REM period nearly 2 minutes early
Journal: Nature Neuroscience (top-tier) | Design: Neuropixels electrophysiology + optogenetics | Model: C57BL/6J mice (n=6 for simultaneous recording; 24 total for connectivity) | Published: May 25, 2026
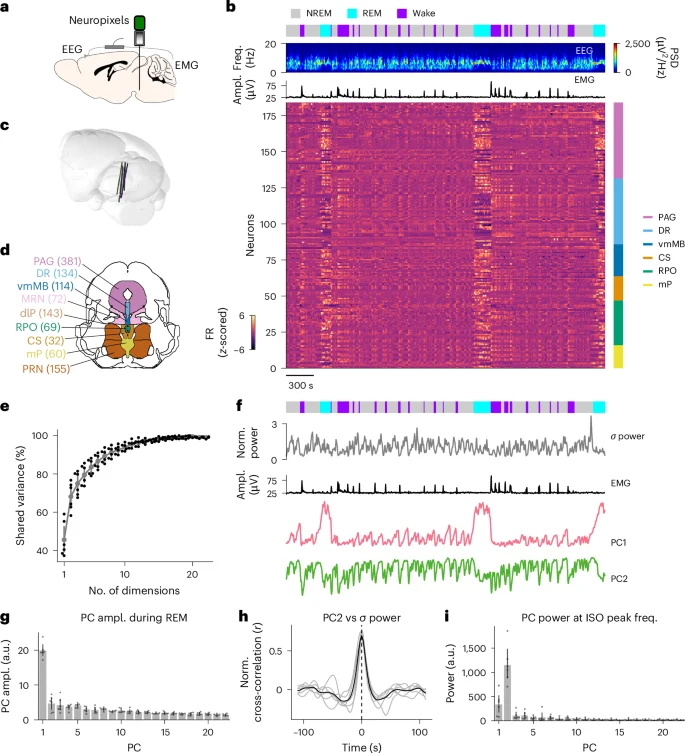
Franz Weber's lab at the University of Pennsylvania recorded 162–226 brainstem neurons simultaneously during sleep and applied principal component analysis to the collective signal. Two components explained 68% of shared variance across the midbrain and pons. 1
The mechanically interesting result: PC2 — an infraslow fluctuation with a period of roughly 10–20 minutes — crossed its threshold and predicted NREM→REM transitions 110 seconds in advance, well before any individual neuron fired reliably. PC1 only became informative at the moment of transition itself. As the authors put it:
"Our results identify a population-level mechanism for gating REM sleep, suggesting that NREM-to-REM sleep transitions are coordinated by low-dimensional, antagonistic brainstem dynamics." 1
The circuit logic involves two antagonistic populations. REM-off neurons (labeled c1−c2−) and REM-on neurons (c1+c2+) ramp against each other across three timescales: synaptic (milliseconds), infraslow (minutes), and ultradian (every 90 minutes across the night). Optogenetic activation of medullary GAD2 REM-on neurons preferentially suppressed REM-off neurons — and crucially, whether that activation actually triggered REM depended on the PC2 state at the moment of stimulation. A high PC2 state at stimulation onset gated whether the upstream circuit could fire REM at all.
The infraslow modulation strength of any given neuron explained 71% of its ultradian ramping slope during inter-REM intervals (r = 0.71). 1 In plain terms: the same slow rhythm that sets up each REM episode also determines how reliably that neuron participates in the next one.
Why it matters for wearable users: REM fragmentation — the thing your Oura or WHOOP scores poorly when you drink alcohol, take sleep aids, or shift your bedtime — may operate through this PC2 gating mechanism. Anything that disrupts the ~10-20 minute infraslow buildup (alcohol suppresses NREM oscillatory depth; most sedatives flatten slow-wave activity; late bedtimes shift the circadian timing of the ultradian cycle) plausibly delays or blocks this PC2 gate. The 110-second prediction window also suggests that future closed-loop devices — ones that can sense and stimulate in real time — could intervene at the population-dynamics level rather than the single-neuron level.
Loading link preview…
Figure 1: Low-dimensional brainstem dynamics gate REM sleep — two principal components capture most of the shared network variance 1
2. Two large wearable datasets document women's sleep disruption in quantified detail
Two independent studies — one using WHOOP, one using Apple Watch — landed in the same week and measured the same phenomenon from different angles. The convergence is worth reading as a single data point.
Study A — WHOOP, 1.2 million device-days: A Stanford Wu Tsai Human Performance Alliance analysis of 2,596 women who collectively logged 42,759 menstrual cycles on WHOOP found that cycle length variability is strongly predicted by how much sleep those women get. Women who averaged 6 hours of sleep showed greater cycle-to-cycle variability than women who averaged 8 hours. 2 In a within-participant natural experiment — effectively isolating the effect on the same person across different weeks — a 10% reduction in weekly sleep duration caused resting heart rate to rise 1.2%, regardless of cycle phase. 2 Nature npj Digital Medicine, May 25, 2026.
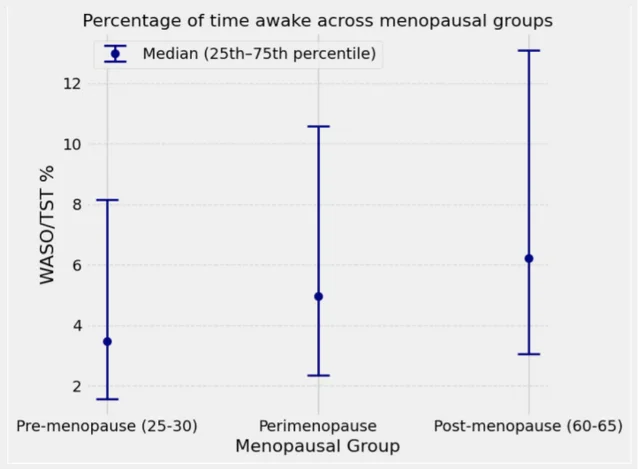
Study B — Apple Watch, 94,118 nights: Harvard's Apple Women's Health Study analyzed tracking data from 338 participants (aged 25–59, majority 45–59) across 94,118 nights. 3 During the 12 months surrounding the final menstrual period, participants spent approximately 0.8% more time awake during sleep — around 4 extra minutes per 8-hour night — compared with the ~0.2% (about 1 extra minute) attributable to simply aging 2 years. In the 18 months leading to menopause, 60% of women with sleep tracking data showed increased wake after sleep onset (WASO), with an average increase of 7%. 3
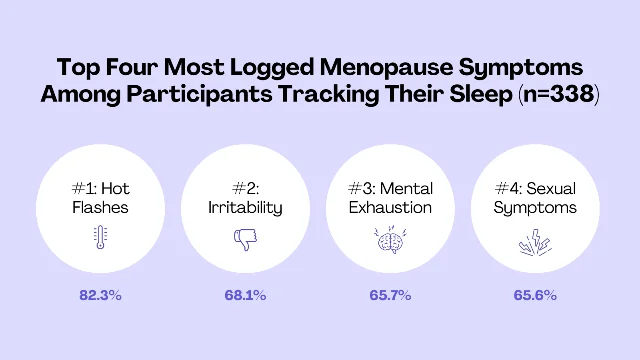
The Harvard team found that individual variation was high — "each person experiences perimenopause and menopause differently" — and that the symptoms most tightly correlated with worsened sleep were not the ones most frequently reported. Hot flashes were the most common symptom (82.3% of participants), but bladder symptoms, joint pain, cardiac discomfort, and depressive symptoms were the strongest independent predictors of worse sleep. 3 4
The practical implication for WHOOP and Apple Watch users is that WASO — not total sleep time — is the metric to watch during perimenopausal transition. A 7% increase in WASO is detectable on both platforms; tracking it monthly around the 40-48 age window gives an early signal that behavioral or clinical intervention may be warranted.
More from the journals
3. Six months of OSA treatment partially restores sleep spindles
Journal: Scientific Reports | Design: Longitudinal observational | N: 216 patients (66 no/mild, 50 moderate, 100 severe OSA) | Published: May 30, 2026
Researchers at Bioaraba Health Research Institute in Spain and Macquarie University measured sleep spindle density (SSD) in OSA patients before and after 6 months of routine clinical management. At baseline, severe OSA patients showed significantly lower SSD than the other groups. After treatment, SSD increased only in the severe group: +0.47 events/minute at the central N2 derivation (95% CI 0.30 to 0.65). After multiple comparison correction, only fast spindles at central derivation remained significant. 5
Sleep spindles are bursts of 12–16 Hz oscillatory activity during NREM sleep, generated by thalamocortical circuits, and associated with memory consolidation and cognitive performance. Their partial recovery after OSA treatment — even in the moderate and mild groups where improvement was not significant — suggests SSD could eventually serve as a microstructural biomarker alongside AHI for tracking treatment response.
4. Walking improves sleep: a Bayesian meta-analysis of 21 RCTs
Journal: Frontiers in Public Health | Design: Bayesian three-level meta-analysis with dose-response modeling | N: 21 RCTs, 1,707 participants, 66 effect sizes | Published: May 28, 2026
The headline number: walking produced a Hedges' g = −0.76 improvement in subjective sleep quality (95% Credible Interval: −0.99 to −0.55), with a Bayes Factor exceeding 10⁵ — classified as extreme evidence by standard interpretation thresholds. 6 The posterior probability of exceeding the minimal clinically important difference was 99.97%. The 95% prediction interval was entirely below zero, meaning the effect is expected to hold positive across new studies.
The strongest moderator was baseline Pittsburgh Sleep Quality Index (PSQI) score (β = −0.297): people who slept worse at the start got more benefit from walking. Supervision mode and exercise environment did not significantly moderate the effect.
The dose model points to: moderate intensity, 3–5 sessions per week, 30–60 minutes per session, for 12–24 weeks. Note the GRADE certainty of evidence is rated very low — the effect size is robust, but most included RCTs had methodological limitations. The effect is on subjective sleep quality (PSQI), not on actigraphy or PSG-measured sleep architecture. 6
5. CBT for menopausal insomnia: a small but positive RCT
Journal: Menopause (via Healio) | Design: Pilot RCT | N: 43 perimenopausal/postmenopausal women | Published: May 27, 2026
Baylor College of Medicine's Sara Nowakowski and colleagues adapted CBT-I for women with both insomnia and vasomotor symptoms (≥1 hot flash per night). The intervention was 4 × 50-minute sessions over 8 weeks, delivered by psychologists, nurses, or social workers — an important feasibility signal for scalability. 7
Results at 1-month follow-up:
| Outcome | CBT group | Control | P value |
|---|---|---|---|
| Insomnia Severity Index | 4.1 | 8.5 | 0.01 |
| No clinically significant insomnia | 69% | 30% | — |
| Hot flash interference score | 0.9 | 2.2 | 0.01 |
| Sleep self-efficacy | 36.8 | 30.5 | 0.01 |
Nowakowski described the goal: "We adapted CBT for insomnia to address both insomnia and nighttime vasomotor symptoms. [The intervention] produced meaningful improvements in insomnia severity, hot flash interference, sleep self-efficacy and depressive symptoms." 7
One limitation: daytime insomnia symptoms did not improve — the authors suggest adding behavioral strategies targeting daytime functioning in future protocols. This is a pilot (n=43) and results require replication, but the effect sizes are large and the delivery model (non-physician providers) is practically attractive.
Wearables and device news
Oura Ring 5 ships June 4 with blood pressure pattern tracking
Oura announced Ring 5 on May 28: 40% smaller than Gen 4, same sensor accuracy, starting at $399, shipping June 4. 8 Alongside the hardware, Oura launched Health Radar — a continuous monitoring layer that alerts users to significant deviations in body temperature, respiratory rate, and, new this cycle, blood pressure patterns during sleep and nighttime breathing disturbances. 9
Oura CEO Tom Hale said the company spent six months testing: "We have finally achieved what I think seems like a real technological miracle. This is what our members have been asking us for, for years." 8
The company has now sold 5.5 million rings, projects roughly $2 billion in 2026 revenue, and has submitted a confidential IPO filing. Also announced: a partnership with Counsel Health for AI-enabled care access in 43 U.S. states, and GLP-1 Insights — dose tracking and side effect logging for patients on GLP-1 medications.
Separately, Oura and Cambridge Cognition (a neuroscience technology company) launched a large-scale brain health study through Oura Labs: up to 45,000 Oura members will complete CANTAB Pathway cognitive assessments (CANTAB One, CANTAB Insight) inside the Oura app while the ring continuously monitors sleep, activity, and stress markers. 10 Oura SVP of Science Shyamal Patel described the study goal: "Cognitive health is one of the least understood frontiers in preventive medicine." 10
WHOOP researchers co-author a jet lag and travel recovery review
WHOOP research scientists, together with collaborators from UCSF, UCLA, Ontario Tech University, Monash University, and Brigham and Women's Hospital, published a peer-reviewed narrative review in Sports Medicine on the physiology of travel fatigue and evidence-based mitigation. 11 The review covers travel's effects on sleep, circadian rhythm, hydration, immune function, cognition, and recovery.
The protocol the review recommends, distilled:
- Pre-travel (3–5 days before): sleep 8–9 hours per night; gradually shift sleep and meal timing ~1 hour per day toward the destination time zone
- During overnight flights: minimize light exposure; avoid alcohol
- Post-arrival: seek natural light at times that advance or delay your clock depending on direction of travel; align meals and activity with local time immediately
From the researchers
Matt Walker launches a clinical sleep platform — and explains why you delay bedtime
Matthew Walker (UC Berkeley; Why We Sleep) made two significant outputs this week. On May 26, Walker formally launched Nightfall IQ, a platform that integrates wearable sleep data with personalized guidance and, through a separate clinical layer called Nightfall RX, connects users with certified sleep physicians for telehealth, pharmacological review, and evidence-based care. 12 Walker positioned the distinction from standard wearable products: "Wearables give us sleep data, but not solutions. Nightfall IQ turns your sleep numbers into intelligent interpretation, personalized guidance, and clinical care. We're a solutions company, not a data company." 13 Alpha testing opened on the same day.
On May 27, Walker released podcast episode #137, focused on bedtime procrastination — the "revenge bedtime" behavior of deliberately delaying sleep to reclaim personal time. Drawing on 43 studies, Walker drew the key clinical distinction: bedtime procrastination is not insomnia. Insomnia is a locked door (you want to sleep but can't). Procrastination is an unlocked door you choose not to walk through. 14 The data from those studies suggests low self-control and chronotype conflict (forced early wake times) are the primary drivers, costing roughly 50 minutes of sleep per night. Walker's framing: "Bedtime procrastination is a small loan from tomorrow. The relief is real. So is the interest: shorter sleep, poorer sleep quality, more fatigue, and worse mood the next day." 14
The solution he describes is based on implementation intentions — "if-then" plans that pre-commit behavior: If it is 10:30 PM and I am watching something, I will finish the current episode and set my phone in the other room. Trials of this technique show it meaningfully reduces the gap between intended and actual bedtime.
Michael Grandner lands a $3.8M NIH grant for sleep-mental health intervention research
Michael Grandner, PhD (University of Arizona, Sleep and Health Research Program) announced this week that his program received a $3.8 million NIH grant to fund research on mind-body sleep interventions. 15 Grandner also published a perspective piece in SLEEP this week arguing that climate change — rising ambient temperatures, disrupted seasonal patterns, extreme weather events — constitutes an urgent and underaddressed threat to population sleep health and demands a new coordinated research agenda. 16
This week's actionable insight: walk 30 minutes to fix the sleep you're already tracking
The walking meta-analysis is worth translating directly into a trackable protocol.
The data: 21 RCTs, 1,707 people, g = −0.76, Bayes Factor > 10⁵, 99.97% probability of exceeding the clinically meaningful threshold. The people who benefited most were those with the worst baseline sleep — exactly the profile of someone whose Oura Readiness or WHOOP Recovery scores are chronically low. 6
The protocol:
- Open your sleep app and find your 30-day PSQI equivalent — Oura's Sleep Score average, WHOOP's Recovery trend, or Apple Health's sleep consistency metric
- If your scores are consistently below your baseline (or if your subjective sleep feels poor), commit to 30–45 minutes of moderate-pace walking, 4 times per week, for 12 weeks
- Moderate pace means you can hold a conversation but not sing — roughly 55–65% of max heart rate, which most wrist devices measure reliably
- Track not just your sleep scores but specifically WASO (time awake after falling asleep) and deep sleep minutes — the walking literature suggests those are the dimensions most likely to move
- At week 12, compare your 7-day average Sleep Score or Recovery to your pre-intervention baseline; a g = −0.76 effect corresponds to roughly a 4–6 point improvement on a 100-point sleep quality scale
The limitation: the outcome measure in all 21 trials is subjective sleep quality (how you feel you slept), not PSG-measured architecture. Your wearable score is a reasonable proxy. The effect likely reflects a combination of reduced arousal, improved sleep pressure from physical exertion, and circadian benefits of morning light exposure during outdoor walks.
Cover image: Fig. 1 from "Low-dimensional population dynamics in the brainstem gate REM sleep," Lozano, Hong, Jin et al. (Weber lab), Nature Neuroscience, May 25, 2026. 1
References
- 1Low-dimensional population dynamics in the brainstem gate REM sleep
- 2The menstrual cycle through the lens of a wearable device
- 3Sleep patterns and changes in perimenopause
- 4Apple Watch sleep data helps Harvard researchers study menopause transition
- 5Sleep spindle density increases after 6 months of OSA treatment
- 6Walking and subjective sleep quality: a Bayesian meta-analysis
- 7CBT may improve insomnia and hot flashes during menopause
- 8Oura is launching its smallest smart ring yet
- 9Introducing Health Radar
- 10Cambridge Cognition and Oura launch brain health study
- 11WHOOP researchers contribute to travel recovery review
- 12Sleep tracking gets clinical
- 13Nightfall IQ launch tweet
- 14#137 – Bedtime procrastination
- 15Michael Grandner: new $3.8M NIH grant
- 16Why climate change demands a new sleep science agenda
Related content
- Sign in to comment.