
2026/6/19 · 9:22
Five papers: June 19, 2026
Five papers from the June 17–19, 2026 window, ranked by journal IF tier and clinical translational signal. HARMONi-A delivers final OS data for ivonescimab (HR 0.74, P=.02) in post-TKI EGFR NSCLC; a Yale/NLM study finds 87% of LLM medical pre-training memorization persists after fine-tuning — a patient-privacy alarm using 13,000+ real EHR records; a JAMA Oncology meta-analysis quantifies second primary malignancies after bispecific antibody therapy at 3.5% pooled; Lancet Psychiatry documents non-specialist psychosocial care benefit across 45 RCTs in violence-exposed populations; and Weizmann Institute maps the brain-to-spleen noradrenergic circuit as a regulator of microglial health in Alzheimer's disease.

研究速览
At a glance — June 19, 2026
| # | Paper | Journal (IF tier) | Design | N | Primary result |
|---|---|---|---|---|---|
| 1 | HARMONi-A: ivonescimab + chemo in EGFR-variant NSCLC | JAMA (IF ~63, T1) | Phase 3 RCT | 322 | Median OS 16.8 vs 14.1 mo; HR 0.74 (P=0.02) |
| 2 | LLM medical data memorization: prevalence and implications | Nat Commun (IF ~16, T2) | Empirical AI safety study | 13,000+ EHR records analyzed | 87% of pre-training memorization persists after fine-tuning |
| 3 | Second primary malignancies after bispecific antibody therapy | JAMA Oncol (IF ~31, T1) | Systematic review & meta-analysis | 2,551 | SPM pooled proportion 3.5% (95% CI 1.8–6.9) |
| 4 | Non-specialist psychosocial care after war and violence | Lancet Psychiatry (IF ~30, T1) | Systematic review & meta-analysis | 9,431 | Anxiety SMD −0.44; PTSD SMD −0.34; all P < 0.0001 |
| 5 | Brain-spleen axis disruption accelerates Alzheimer's disease | Nat Commun (IF ~16, T2) | Translational (5xFAD + retinal injury mouse) | — | Splenic denervation → ↓ monocyte recruitment → ↓ microglial DAM transition → ↑ cognitive decline |
正在加载统计卡片…
Ranked by journal IF tier and clinical translational signal. Coverage window: June 17–19, 2026 (PubMed indexing dates; 5 papers previously published June 18 are excluded). No new original research appeared in NEJM, The Lancet (main), or Nature Medicine during this window.
1. HARMONi-A final OS: ivonescimab plus chemotherapy improves survival after EGFR-TKI failure in NSCLC (JAMA, IF ~63)
Journal: JAMA · IF ~63, Tier 1 · Published June 17, 2026 · DOI: 10.1001/jama.2026.7745 · PMID: 42307937 · ClinicalTrials.gov: NCT05184712
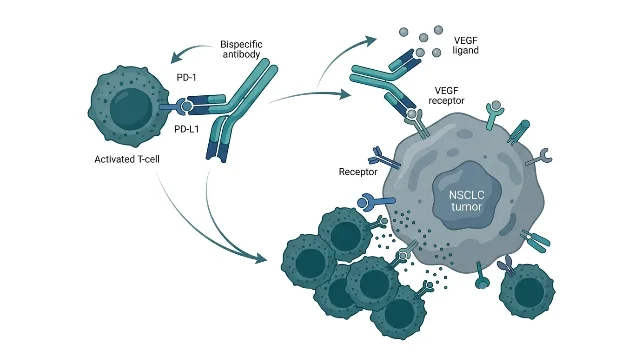
Design: Phase 3, double-blind, placebo-controlled RCT. 55 sites in China. 322 patients with EGFR-variant (exon 19 deletion or L858R) nonsquamous NSCLC who had progressed after prior EGFR tyrosine kinase inhibitor (TKI) therapy. Enrollment: January–November 2022; data cutoff: April 12, 2025. This report covers the final overall survival (OS) analysis — the primary PFS endpoint was previously published (JAMA 2024;332:561–570). First author: Wenfeng Fang (Sun Yat-sen University Cancer Center). Senior/corresponding: Li Zhang (Sun Yat-sen University Cancer Center). Funding/COI: Akeso Biopharma (manufacturer of ivonescimab) had employees among authors (M. Xia, D. Lu, M.Y. Xia). 1
Ivonescimab is a bispecific antibody that simultaneously targets PD-1 (programmed cell death protein 1) and VEGF (vascular endothelial growth factor), combining immune checkpoint inhibition with anti-angiogenic activity in a single molecule. 1
Primary OS finding: Median OS 16.8 months (ivonescimab + pemetrexed/carboplatin) vs 14.1 months (placebo + pemetrexed/carboplatin). Stratified HR 0.74 (95% CI, 0.58–0.95; P = .02). Absolute median OS difference: 2.7 months. 1
30-month landmark survival: 29.1% (95% CI, 22.1–36.4%) in the ivonescimab arm vs 18.4% (95% CI, 12.8–24.8%) in the placebo arm — a 10.7 percentage-point absolute difference at 30 months. 1
Safety: Grade ≥3 treatment-emergent adverse events occurred in 67.1% of the ivonescimab arm vs 54.7% in the placebo arm. The toxicity increment is clinically real and relevant for patient selection. 1
The authors' stated conclusion: "Ivonescimab plus chemotherapy provided a statistically significant and clinically meaningful improvement in overall survival with an acceptable safety profile." 1
Clinical implication: This is the OS readout for a PD-1/VEGF bispecific antibody in a line of therapy — post-EGFR-TKI NSCLC — where pembrolizumab monotherapy has limited activity. The HR 0.74 is modest but statistically secure, and the 30-month separation (29.1% vs 18.4%) is clinically meaningful for a population where long-term survival is historically rare. Three caveats matter before extrapolating: the trial was conducted entirely in China, enrolled only EGFR exon 19 del/L858R variants, and carries Akeso Biopharma authorship — all standard considerations for assessing generalizability. Ivonescimab does not yet have FDA or EMA approval in this indication; regulatory filings will be the next readout. Thoracic oncologists tracking the post-third-generation TKI space should log this as the current best OS evidence for a bispecific checkpoint-plus-anti-angiogenic combination in this patient population.
2. LLM medical data memorization: 87% of pre-training content persists after fine-tuning, including real patient records (Nature Communications, IF ~16)
Journal: Nature Communications · IF ~16, Tier 2 · Open Access CC BY-NC-ND 4.0 · Published June 19, 2026 · DOI: 10.1038/s41467-026-73779-6
Design: Empirical AI safety/privacy study. Three adaptation scenarios analyzed: (1) continued pretraining on medical corpora, (2) fine-tuning on standard medical benchmarks, (3) fine-tuning on real-world clinical data including 13,000+ unique inpatient records from Yale New Haven Health System. 21 authors across Yale School of Medicine, National Library of Medicine (NIH/NLM), Imperial College London, UTHealth Houston, UC San Diego, Vanderbilt, and the National University of Singapore. NIH-funded (grant 1R01LM014604, NLM Intramural Research Program). Corresponding author: Qingyu Chen (Yale). 2
Key finding: The study found that "memorization is prevalent and significantly higher than that in the general domain," and that "up to 87% of content memorized during continued pretraining remains after fine-tuning" — meaning fine-tuning alone does not erase sensitive content that a model has absorbed during pretraining. 2
Three memorization categories identified: 2
- Beneficial: accurate recall of clinical guidelines, evidence-based protocols
- Uninformative: templated boilerplate language with no clinical signal
- Harmful: sensitive clinical content capable of compromising patient privacy — the primary concern when real EHR data is used for LLM training
Clinical implication: This paper has two separate audiences. For healthcare AI developers: the 87% persistence figure means that privacy guarantees cannot rest on fine-tuning stage alone — differential privacy, data curation standards, or selective forgetting mechanisms need to operate at the pretraining stage or within the training data itself. For clinicians and privacy officers evaluating hospital-AI vendor contracts: any LLM whose pretraining or continued pretraining touched real patient records is subject to the memorization risk this study quantifies. The Yale New Haven dataset use here is disclosed in the paper, but the same phenomenon applies to commercial models trained on proprietary clinical data. The authors provide practical recommendations for each memorization category, and this paper is likely to be cited in upcoming FDA and EU AI Act guidance on healthcare LLM safety requirements.
3. Second primary malignancies after T-cell–engaging bispecific antibody therapy: 3.5% pooled rate at median 17 months (JAMA Oncology, IF ~31)
Journal: JAMA Oncology · IF ~31, Tier 1 · Published June 18, 2026 · DOI: 10.1001/jamaoncol.2026.1859 · PMID: 42313425 · PROSPERO: registered
Design: Systematic review and meta-analysis. Data sources: PubMed and Embase through October 1, 2025. From 494 records screened, 20 studies (26 cohorts; N = 2,551 patients) met inclusion criteria — encompassing B-cell non-Hodgkin lymphoma (NHL) and multiple myeloma (MM) patients treated with T-cell–engaging bispecific antibodies (BsAbs), including agents such as mosunetuzumab, glofitamab, epcoritamab, odronextamab, teclistamab, and talquetamab. Median follow-up: 17.4 months (range 5.7–25.6). First author: Jaromir Tomasik (Medical University of Warsaw). Senior/corresponding: Kai Rejeski (LMU University Hospital Munich / Memorial Sloan Kettering Cancer Center). Additional affiliations: NYU Langone, Peter MacCallum Cancer Centre, Vall d'Hebron, Dana-Farber, Rabin Medical Center. 3
Primary pooled estimate — total SPM proportion: 3.5% (95% CI, 1.8–6.9) across 20 studies. 3
Disease-specific estimates: NHL: 3.8% (95% CI, 2.3–6.3); MM: 3.4% (95% CI, 0–76.7 — wide CI reflecting small MM-specific cohort heterogeneity). 3
Clinical severity: SPMs leading to treatment discontinuation: 2.2% (95% CI, 1.5–3.1). SPMs leading to death: 1.4% (95% CI, 1.1–1.9). 3
Exploratory meta-regression: No study-level covariates — follow-up duration, disease category, prior therapy lines, or patient age — were associated with total SPM estimates. This means clinicians cannot currently risk-stratify individual patients for SPM based on these variables. 3
The authors' stated conclusion: "Despite relatively short follow-up, SPMs were a measurable and clinically relevant complication of BsAb therapy," with heterogeneous reporting across studies complicating comprehensive safety assessment. 3
Clinical implication: BsAb therapies for B-cell NHL and MM have entered routine practice following approvals across multiple agents since 2022, and the number of patients with meaningful follow-up is now sufficient to estimate rare events like SPMs. A 3.5% pooled rate at 17 months — with 1.4% fatal SPMs — is not negligible for a patient population that may be approaching long-term remission. The limitation is real: median follow-up of 17 months undercounts late-appearing malignancies, and the MM meta-regression CI (0–76.7%) reflects a dataset that cannot yet give stable estimates for that subgroup. For oncologists managing BsAb-treated patients in follow-up, the practical implication is surveillance: the field currently lacks standardized reporting criteria for post-BsAb SPMs, and this paper makes a direct argument for including standardized long-term oncologic surveillance protocols in BsAb clinical trials and post-approval registries.
4. Non-specialist psychosocial care after war and interpersonal violence: small-to-moderate benefit across 45 RCTs (Lancet Psychiatry, IF ~30)
Journal: The Lancet Psychiatry · IF ~30, Tier 1 · Published July 1, 2026 (PubMed-indexed June 17–18, 2026) · DOI: 10.1016/S2215-0366(26)00123-9 · PMID: 42309105 · PROSPERO: CRD42022306099
Design: Systematic review and meta-analysis. Seven databases searched from January 1, 2000 to June 1, 2025. From 54,748 abstracts screened, 45 eligible RCTs were identified, enrolling 9,431 participants (mean age 37.9 years). Exposures: war/armed conflict or interpersonal violence (IPV). Interventions: psychosocial care delivered by non-specialists — task-shared delivery from trained community members, lay workers, or community health workers, rather than licensed mental health clinicians. First author: Anushka R. Patel (Harvard T.H. Chan School of Public Health). Corresponding: Abhijit Nadkarni (London School of Hygiene & Tropical Medicine / Sangath, Goa, India). Funding: NIH Training Grant (5T32MH017119-36), EU Horizon-MSCA, NIHR Global Health Research Professorship (NIHR302421). 4
Primary outcomes (all P < 0.0001): 4
| Outcome | SMD | 95% CI |
|---|---|---|
| Anxiety | −0.44 | −0.57 to −0.32 |
| Depression | −0.41 | −0.51 to −0.31 |
| PTSD | −0.34 | −0.44 to −0.24 |
| Functional impairment | −0.34 | −0.47 to −0.22 |
Sensitivity analyses: SMD range −0.30 to −0.55, all P < 0.0001. 4
Subgroup findings: Strongest effects in refugee populations. Veterans showed non-significant results across all outcomes. Depression and anxiety outcomes were non-significant in interpersonal violence survivors specifically. Transdiagnostic treatments (addressing multiple symptom clusters simultaneously) showed benefit across all four outcomes. 4
Heterogeneity and quality: Between-study heterogeneity I² = 77–84% across outcomes — high, reflecting the diversity of interventions, settings, and populations. 98% of studies had some risk of bias. The authors characterized effects as "small to moderate clinical benefits" and noted these findings "can inform psychosocial programming related to setting, providers, types of violence, and treatment foci." 4
Clinical implication: The policy relevance here is substantial and explicit. Globally, the ratio of mental health professionals to population in conflict-affected and low-resource settings makes specialist-only care models functionally undeliverable. SMDs of −0.34 to −0.44 are clinically meaningful in this context — comparable to effect sizes from pharmacotherapy in depression trials at the population level. The differential by population (refugees benefit, veterans do not with current evidence) and by violence type (IPV survivors show weaker signal) is the operationally important result: implementing organizations should not apply a one-size-fits-all program design. The high I² (77–84%) and near-universal risk-of-bias flags are honest limitations, but the 45-RCT, 9,431-participant evidence base is the largest assembled for this intervention class and provides a defensible foundation for WHO and UNHCR program scaling decisions.
5. Brain-spleen neural axis maintains microglial health in Alzheimer's disease: disruption accelerates cognitive decline (Nature Communications, IF ~16)
Journal: Nature Communications · IF ~16, Tier 2 · Open Access CC BY-NC-ND 4.0 · Published June 19, 2026 · DOI: 10.1038/s41467-026-74253-z
Design: Translational study. Primary model: 5xFAD transgenic mouse model of amyloidosis (modeling Alzheimer's disease). Retrograde neuronal tracing used to map brain-spleen connectivity. Interventions: splenic nerve denervation at early presymptomatic stage; pharmacological enhancement of splenic noradrenergic input. Secondary validation: retinal cytotoxic injury model. Corresponding authors: Tommaso Croese, Naomi Habib, and Michal Schwartz (Weizmann Institute of Science, Rehovot, Israel; Hebrew University of Jerusalem). Funding: European Research Council Advanced Grant, Israel Science Foundation, Chan Zuckerberg Initiative, Myers Foundation. Competing interest: Michal Schwartz is co-founder and CSO of ImmunoBrain. 5
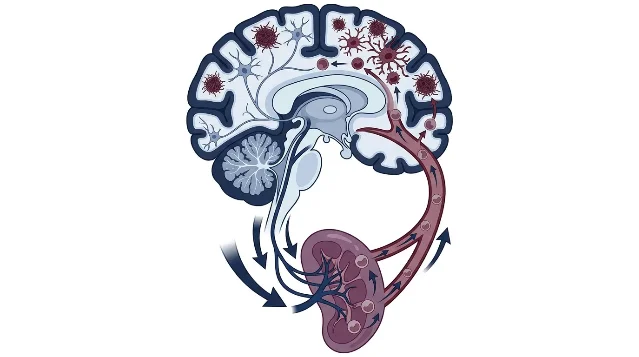
Core mechanism identified: Retrograde tracing at advanced amyloidosis stages revealed reduced brain-to-spleen connectivity. When splenic nerve denervation was induced at an early presymptomatic stage, the following cascade was documented: 5
- Impaired splenic hematopoiesis (reduced production of peripheral monocytes)
- Diminished monocyte recruitment to the brain
- Reduced microglial transition to the disease-associated microglia (DAM) state — the activated, amyloid-clearing phenotype
- Accelerated cognitive decline
The reverse intervention — enhancing splenic noradrenergic input — increased hematopoiesis, restored monocyte homing to brain tissue, and delayed cognitive impairment. The mechanism was independently validated in a retinal cytotoxic injury model, where splenic denervation impaired post-injury survival of retinal ganglion cells. 5
The authors concluded that these findings "identify an active brain–spleen circuit in regulating monocyte recruitment, and establish peripheral monocytes as important drivers of microglial state transitions and disease progression." 5
Clinical implication: The direct therapeutic implication is the splenic noradrenergic axis as a drug target upstream of microglial activation in Alzheimer's disease. Adrenergic pharmacology (including agents already in clinical use, such as norepinephrine reuptake inhibitors or α/β agonists) has not been systematically explored for modulating this peripheral-to-central immune axis. The Schwartz lab's neuroimmune research history — including prior work establishing that T-cell trafficking through the choroid plexus is neuroprotective — gives this mechanistic finding credibility as more than isolated mouse data. The ImmunoBrain competing interest is worth noting given the therapeutic direction, but does not alter the mechanistic logic. The retinal ganglion cell cross-validation in a separate injury model extends the principle beyond Alzheimer's to neurodegeneration more broadly. The gap between these mouse findings and a human clinical target is large — no human data are reported, and the 5xFAD model overexpresses amyloid mutations not typical of sporadic Alzheimer's — but for neuroscience researchers tracking peripheral immune contributions to CNS disease, this axis is now backed by a rigorous causal intervention dataset from a top-tier neuroimmunology group.
Cover image: photo by Chokniti Khongchum via Pexels (royalty-free).
参考来源
- 1PubMed — HARMONi-A ivonescimab + chemotherapy in EGFR NSCLC, final OS
- 2Nature Communications — LLM medical data memorization: prevalence, characteristics, and implications
- 3PubMed — Second primary malignant neoplasms after T-cell–engaging bispecific antibody therapy
- 4PubMed — Non-specialist psychosocial care after war and interpersonal violence
- 5Nature Communications — Brain-spleen axis disruption accelerates Alzheimer's disease via monocyte-microglia failure


围绕这条内容继续补充观点或上下文。