2026/6/26 · 7:20
Summer did not fix vitamin D levels
A new European Journal of Clinical Nutrition screening study found that vitamin D insufficiency stayed high among older adults and adults with darker skin in northern Britain, even during summer. The practical takeaway is to treat vitamin D as a year-round intake issue for higher-risk groups and follow the 10 micrograms/day guidance rather than stopping supplementation when the weather improves.

研究速览
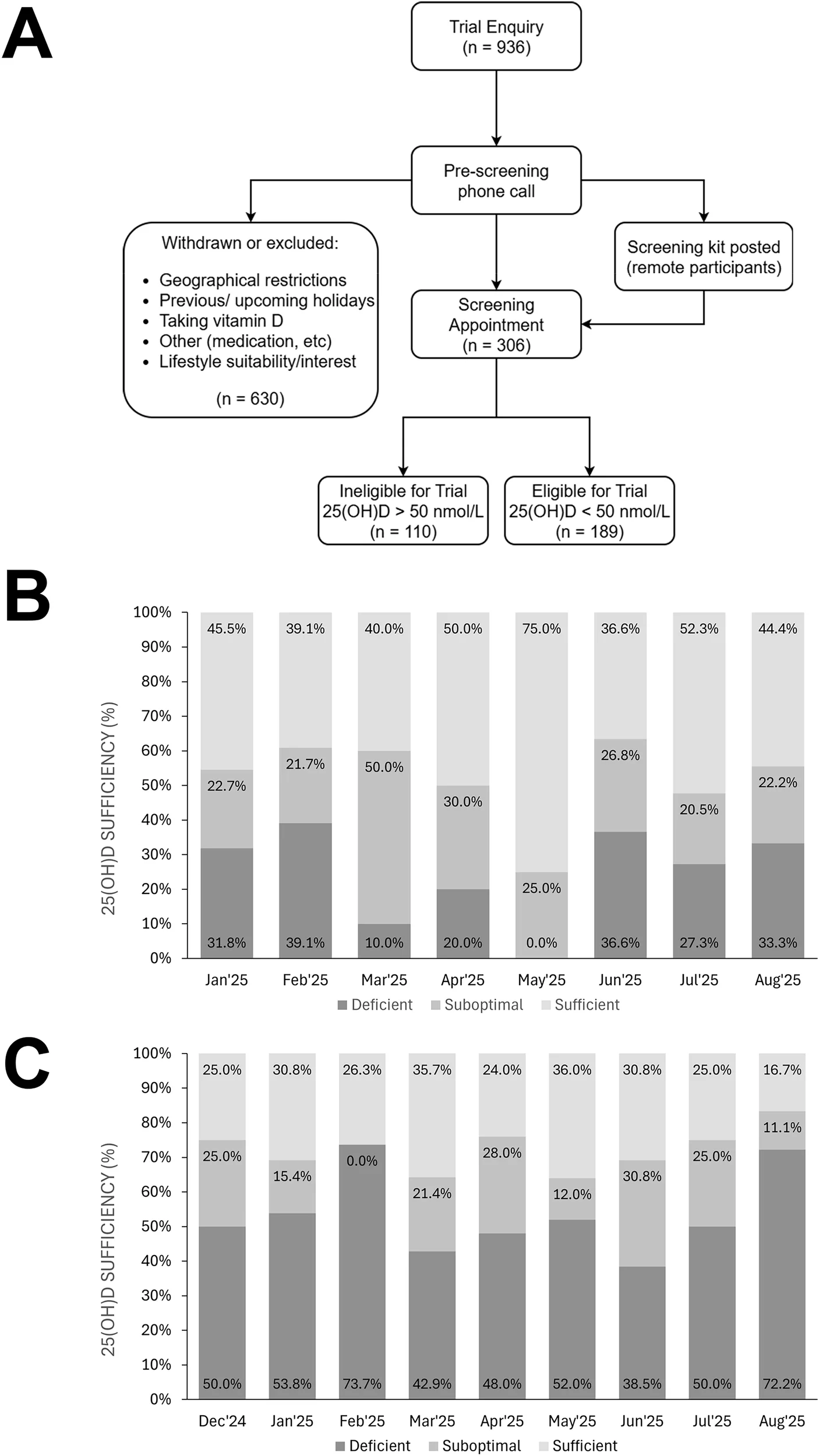
For older adults and people with darker skin living in northern Britain, the practical vitamin D rule from a new European Journal of Clinical Nutrition paper is blunt: do not wait for summer sunlight to do the job. In screening data from 299 adults, 54.8% of participants aged 65 or older and 72.1% of adults with Fitzpatrick IV-VI skin types had 25(OH)D below 50 nmol/L, the paper's threshold for insufficiency or deficiency. 1
The surprise is the seasonality result. Among the older-adult group, insufficiency still averaged 55.6% during June-August 2025, and the ethnic-minority group showed no clear improvement across winter, spring, or summer. 1 That makes this less a story about a nutrient deficiency in winter and more a warning about assuming that summer corrects risk.
This was not a randomized supplement trial. It was a cross-sectional screening analysis from the recruitment phase of clinical trial ISRCTN13778806, so it can describe prevalence and season patterns but cannot prove that supplementation would change outcomes in this sample. 1 The dietary takeaway is still actionable because it lines up with existing UK guidance: adults in higher-risk groups should consider 10 micrograms of vitamin D per day throughout the year. 2
What the study actually measured
Goddard, Watson, Tilbury, Corfe, and Fairley screened 299 adults in northern Britain between December 2024 and August 2025. The analysis included 168 adults aged 65 or older and 147 adults aged 18 or older with Fitzpatrick IV-VI skin types, with about 16 people overlapping between the two groups. 1 The older-adult group was free-living rather than living in care homes or sheltered accommodation, which matters because care-home residents often have even less sun exposure. 1
The researchers used dried blood spot finger-prick samples and LC-MS/MS analysis by SureScreen Scientifics Ltd in Derby. They defined vitamin D sufficiency as 25(OH)D above 50 nmol/L, insufficiency as 31-49 nmol/L, and deficiency as below 30 nmol/L; only 0.67% of samples were below the assay's limit of detection. 1
The headline numbers are easy to misread unless the denominator is clear:
| Group screened | Main finding | Why it matters |
|---|---|---|
| Adults aged 65+ | 54.8% had 25(OH)D below 50 nmol/L, with little month-to-month variation. 1 | The result challenges the common assumption that summer sun reliably restores vitamin D in older adults. |
| Adults with Fitzpatrick IV-VI skin types | 72.1% had 25(OH)D below 50 nmol/L, with no seasonal improvement across winter, spring, or summer. 1 | Darker skin reduces cutaneous vitamin D synthesis, so northern latitude plus skin phenotype can keep risk high year-round. 3 |
| Peak summer months | Older adults still averaged 55.6% insufficiency during June-August 2025. 1 | The relevant decision is year-round intake, not a winter-only supplement habit. |
Mean 25(OH)D was also lower in the ethnic-adult group than in the older-adult group: 40.3 +/- 29.1 nmol/L versus 49.7 +/- 25.9 nmol/L, a mean difference of -9.41 nmol/L. 1 The study did not extract exact monthly percentages for every bar in the figure, so the safest interpretation is the reported pattern, not a month-by-month ranking.
Why summer was the important test
Vitamin D advice often turns into a seasonal habit: take a tablet in winter, relax in summer. This paper directly tests the weak point in that habit. If summer sunlight were enough for these groups, the prevalence of low 25(OH)D should have fallen when daylight and ultraviolet B exposure increased.
That did not happen. The lowest monthly prevalence reported in the study never fell below 25.0% among older adults and never fell below 64.0% among the ethnic-adult group. 1 Prof Bernard Corfe of Newcastle University put the point plainly in the university press release: "What's striking about these findings is that vitamin D levels didn't improve, even in the summer months when we would usually expect them to recover." 4
The result also fits older UK Biobank analyses. Darling et al. reported that 92% of 6,433 UK South Asian adults had 25(OH)D below 50 nmol/L, while Vearing et al. reported that about 78% of 4,046 British African-Caribbean adults were below that threshold. 5 6 The new EJCN paper adds a narrower but more immediately practical point: the risk persisted through summer in a current northern-Britain screening sample.
The dose is boring, and that is the point
The actionable dose is not high. The UK Scientific Advisory Committee on Nutrition recommends a Reference Nutrient Intake of 10 micrograms per day of vitamin D for people aged 4 years and older, including pregnant and lactating women and groups at increased risk of deficiency. 3 The NHS gives the same practical advice for people who are not often outdoors, people in care homes, people who cover most of their skin outdoors, and people with dark skin: consider a daily supplement containing 10 micrograms of vitamin D throughout the year. 2
For shoppers, 10 micrograms is 400 IU. The NHS upper safety limit for adults is 100 micrograms per day, or 4,000 IU, and the lower routine dose is the relevant one for ordinary supplementation unless a clinician has prescribed otherwise. 2
Food can contribute vitamin D, especially oily fish, eggs, fortified foods, and some mushrooms exposed to ultraviolet light. 2 But the study's message is not that food choice should become complicated. For the specific high-risk groups in this paper, a small daily supplement is a more reliable baseline than trying to infer vitamin D status from the calendar.
How much confidence should you put in it?
This finding deserves attention, but it should be used with the right boundaries.
First, the design was cross-sectional. The paper measured vitamin D status at screening; it did not randomize participants to year-round supplementation versus no supplementation and then measure health outcomes. 1 Second, the sample was geographically specific to northern Britain, and the findings may not transfer cleanly to lower-latitude regions with different sunlight exposure, diet, fortification patterns, or supplement habits. 1
Third, the screening funnel may have shaped the sample. Of 936 people who approached the study, 630 were excluded, most commonly because they were already taking cholecalciferol supplements or withdrew because of disinterest or lifestyle constraints. 1 That means the final screened group may underrepresent people who were already successfully supplementing.
The funding disclosure also belongs in the interpretation. The study was funded by BetterYou, a supplement manufacturer, although the paper states that the sponsor was not involved in study design, delivery, or interpretation and that the research was undertaken by Newcastle University. 1 That disclosure does not invalidate the measurements, but it is a reason to keep the recommendation tied to independent public guidance rather than to any branded product.
The dietary decision
If you are over 65, have darker skin, live at a northern latitude, rarely go outdoors, cover most of your skin outdoors, or advise patients in those categories, treat vitamin D as a year-round intake problem.
The practical move is simple: take 10 micrograms (400 IU) of vitamin D daily throughout the year, unless your clinician has given you a different plan. 2 Do not use summer as the signal to stop if you are in one of the higher-risk groups studied here. The new paper's main contribution is that summer did not rescue vitamin D status in the very groups most likely to assume that it might. 1
For dietitians, the counseling script can be short: identify whether the person fits an at-risk category, ask about current supplement use, and confirm whether the routine dose matches the 10-microgram daily guidance. 2 The evidence does not require a complicated food tracking protocol; it supports a boring daily habit that does not change with the month.
Cover image: Figure 1 from Goddard et al., European Journal of Clinical Nutrition (2026), used under CC BY 4.0 from the original article.
相似内容

Your summer bedtime is lying to you. Here's how to stop late sunsets and scrolling from stealing sleep.
Gen Z Health Daily文章
Your weather app's UV number matters more than how hot it feels. Here's how to use it.
Gen Z Health Daily文章
The FDA just approved the first new sunscreen ingredient in 25 years. Here's what actually changed.
Gen Z Health Daily文章
围绕这条内容继续补充观点或上下文。