2026/6/30 · 9:19
Acetaminophen leads June 30 papers
A shortened-window weekly PubMed digest led by a sibling-matched acetaminophen pregnancy study, plus infigratinib, ReMIND T cells, TBI biomarker caveats, and OPTIMUM low-back-pain results.

This issue covers the shortened post-cadence-change PubMed tracking window from June 28 09:21 to June 30 09:00 ET. The ranking reads as a weekly-style top five, but the actual evidence window is just under 48 hours because the channel moved to a Tuesday weekly cadence after the prior issue.
Ranking is based on journal tier, design strength, sample size, clinical decision value, and whether the paper reports quantitative primary findings. Newly indexed papers do not yet have mature citation momentum in the source package, so early citation velocity is not used as a decisive tiebreaker here.
At a glance
| # | Paper | Journal / impact tier | Design | N | Open/read decision |
|---|---|---|---|---|---|
| 1 | Prenatal acetaminophen and ASD/ADHD | JAMA Internal Medicine / top general-internal medicine | Population-based sibling-matched cohort | 124,333 for ASD; 97,285 for ADHD | Open if you counsel pregnancy medication use: sibling-matched analyses found no association with ASD or ADHD, with aHR 1.00 for ASD and 1.01 for ADHD. 1 |
| 2 | Oral infigratinib in achondroplasia | New England Journal of Medicine / highest clinical tier | Phase 3 double-blind RCT | 114 children | Open if you follow pediatric endocrinology or skeletal dysplasia: once-daily oral infigratinib increased annualized height velocity by 1.74 cm/year versus placebo at 52 weeks. 2 |
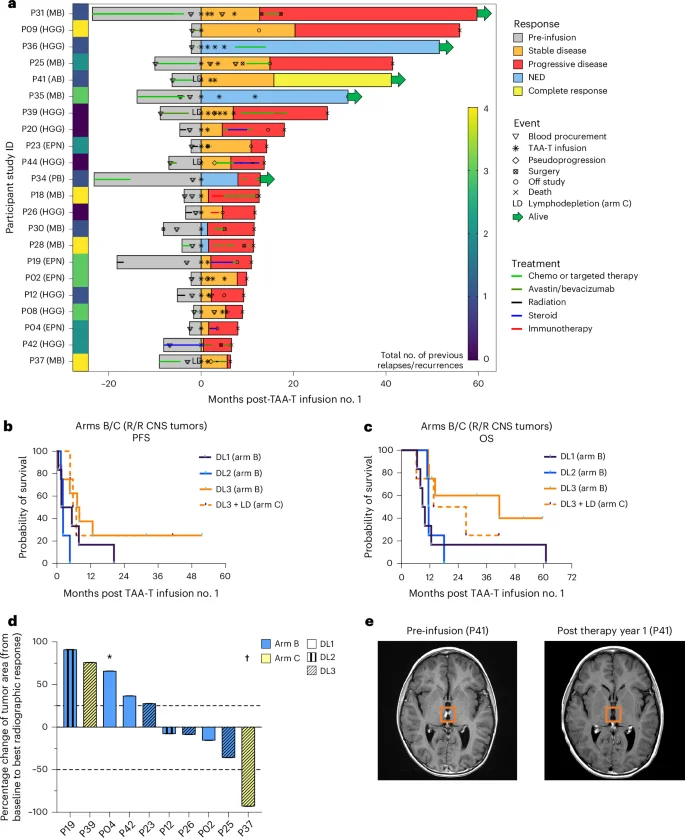
| 3 | ReMIND multi-antigen T cells for pediatric CNS tumors | Nature Medicine / top translational medicine | Phase 1 adaptive dose-finding trial | 51 enrolled; 33 infused | Open for the durable-response signal, but keep the phase 1 denominator visible: three patients in relapsed/refractory arms were alive without disease at 31.8, 41.2, and 51.6 months. 3 |
| 4 | TBI history and Alzheimer blood biomarkers | JAMA Neurology / top specialty tier | Cross-sectional diagnostic test study | 272 veterans | Open before applying plasma p-tau217/Aβ42 results to patients with TBI history: accuracy fell from 90% without TBI to 63% with loss of consciousness over 5 minutes. 4 |
| 5 | Mindfulness group medical visits for chronic low back pain | JAMA Internal Medicine / top general-internal medicine | Pragmatic randomized clinical trial | 451 adults | Open for a scalable care-model signal, not a large analgesic effect: PEG improvement was statistically better than usual care, but the between-group difference did not meet the prespecified 1-point MCID. 5 |
1. Prenatal acetaminophen: sibling matching removes the ASD/ADHD signal
Paper link: PubMed record
What the paper did. S. Luo and E.Y.F. Wan of the University of Hong Kong report a population-based sibling-matched cohort study using Hong Kong electronic health records from 2001 to 2023. The analysis included 124,333 children for autism spectrum disorder and 97,285 children for attention-deficit/hyperactivity disorder after starting from an initial cohort of 708,020 mother-child pairs. 1
Decision signal. In the sibling-matched analyses, prenatal acetaminophen exposure was not associated with autism spectrum disorder, with adjusted HR 1.00 and 95% CI 0.91-1.11, or attention-deficit/hyperactivity disorder, with adjusted HR 1.01 and 95% CI 0.93-1.08. 1 Null findings were consistent across exposure timing, cumulative dose, and sporadic, intermittent, or persistent use patterns. 1
Evidence strength. The paper is ranked first because it addresses a common counseling question with a large design that directly tests familial confounding. Conventional cohort analyses and negative-control analyses of pre-pregnancy exposure both showed positive associations, including HR 1.12 for ASD and HR 1.24 for ADHD in the pre-pregnancy negative control, which supports the authors' interpretation that earlier signals likely reflected residual familial confounding. 1
Clinical implication. The finding supports reassurance for indicated paracetamol or acetaminophen use during pregnancy while preserving the usual principle of using needed medications at appropriate doses. The paper does not argue for unnecessary exposure; it narrows the neurodevelopmental-risk concern that has complicated patient counseling.
2. Infigratinib: an oral phase 3 signal in achondroplasia
Paper link: PubMed record
What the paper did. R. Savarirayan of Murdoch Children's Research Institute and colleagues ran PROPEL 3, a multicenter double-blind placebo-controlled phase 3 trial of oral infigratinib in children with achondroplasia. The trial randomized 114 children aged 3 to 17 years in a 2:1 ratio to infigratinib 0.25 mg/kg or placebo once daily for 52 weeks. 2
Decision signal. At week 52, infigratinib increased annualized height velocity by a least-squares mean between-group difference of 1.74 cm/year, with 95% CI 1.31-2.17 and P<0.001. 2 Height Z-score improved by 0.32, with 96% CI 0.23-0.41 and P<0.001, while the upper-to-lower body segment ratio changed by -0.02, with 96% CI -0.06 to 0.01. 2
Evidence strength. The trial has the strongest journal tier in this issue and a randomized phase 3 design. Adverse events occurred in 96% of the infigratinib group and 95% of the placebo group, serious adverse events occurred in 5% and 3%, and no treatment-related discontinuations were reported. 2 The trial was funded by BridgeBio Pharma. 2
Clinical implication. For clinicians and trialists in skeletal dysplasia, the important distinction is route and evidence phase. Infigratinib is presented in the source package as the first oral FGFR1-3 inhibitor to show significant height-velocity improvement in a phase 3 achondroplasia trial. 2 The remaining decision questions are comparative positioning, long-term proportionality outcomes, and durability beyond the 52-week primary endpoint.
3. ReMIND: durable responses from multi-antigen T cells, still phase 1
Paper link: Nature Medicine full text
What the paper did. Stephanie Gomez, Eugene I. Hwang, and colleagues at Children's National Hospital report ReMIND, an open-label phase 1 adaptive dose-finding trial of multi-antigen-targeting T cells for pediatric central nervous system tumors. The trial enrolled 51 patients and infused 33 across three arms: newly diagnosed DIPG without lymphodepletion, relapsed or refractory nonbrainstem CNS tumors without lymphodepletion, and the same relapsed or refractory setting with fludarabine/cyclophosphamide lymphodepletion. 3
Decision signal. The TAA-T cells targeted WT1, PRAME, and survivin, and 85.4% of procured products, or 41 of 48, were manufactured at dose level 1 or higher. 3 Safety, feasibility, and maximum tolerated dose endpoints were met, with the maximum tolerated dose set at dose level 3, or 8 × 10^7 cells/m² per dose. 3
Evidence strength. The signal sits in the responder tail, not in a randomized comparison. Arm A had median overall survival of 13.7 months from diagnosis, and arms B/C had median progression-free survival of 5.0 months from infusion. 3 Three patients in arms B/C were alive without disease at 31.8, 41.2, and 51.6 months without further treatment, including one complete response. 3 One grade 5 dose-limiting toxicity occurred in a DIPG patient with hydrocephalus, tumor edema, and respiratory failure, and grade 3 or higher treatment-emergent adverse events occurred in 9%, or 3 patients. 3
Research implication. This is the paper to open for pediatric neuro-oncology cell-therapy trial design, especially if manufacturing feasibility and multi-antigen targeting are the decision points. It is not yet a practice-changing efficacy trial; the durable complete-response signal needs confirmation in a later-phase design with a clearer comparator.
4. TBI history: a warning label for Alzheimer blood-test interpretation
Paper link: PubMed record
What the paper did. Y. Rosen-Lang, R.C. Gardner of UCSF and the San Francisco VA, and colleagues conducted a cross-sectional diagnostic test study in the ADNI-DOD cohort. The study included 272 Vietnam War veterans, 99.3% of whom were male, with mean age 70 years. 4
Decision signal. The plasma p-tau217/Aβ42 ratio detected amyloid-PET positivity with 90% accuracy in veterans without traumatic brain injury history, with 95% CI 84%-96%. 4 Accuracy dropped to 78% among veterans with loss of consciousness for 0 to 5 minutes and to 63% among veterans with loss of consciousness for more than 5 minutes, with P=0.03 and P<0.001 versus no TBI. 4 The authors state that the test may miss more than half of amyloid-PET-positive cases in veterans with TBI history. 4
Evidence strength. The paper is not ranked because of sample size alone; it is ranked because plasma Alzheimer biomarkers are moving toward clinical deployment, and this study identifies a specific context where test performance may degrade. The funding source was Department of Defense ADNI and ADBI. 4
Clinical implication. For memory clinics and systems building blood-biomarker pathways, TBI history should be treated as an interpretation variable rather than background trivia. The study population is narrow, so the cleanest implication is caution in veteran and TBI-exposed populations, not abandonment of plasma p-tau217/Aβ42 testing.
5. OPTIMUM: statistically positive mindfulness visits, below the MCID
Paper link: PubMed record
What the paper did. N.E. Morone of Boston University and the University of Pittsburgh and colleagues ran OPTIMUM, a pragmatic randomized clinical trial in adults with chronic low back pain. The study randomized 451 adults, 70.5% female, in a 1:1 ratio to an 8-week telehealth mindfulness group medical visit program or usual care at clinics in Massachusetts, Pennsylvania, and North Carolina from May 2021 to November 2024. 5
Decision signal. At 6 months, the intervention group improved by -1.21 points on the PEG scale, with 95% CI -1.50 to -0.92, versus -0.59 points with usual care, with 95% CI -0.86 to -0.31. 5 The between-group difference was -0.62 points, with 95% CI -1.02 to -0.23 and P=0.002. 5 Effects were also statistically significant at 8 weeks and 12 months, with between-group differences of -0.89 and -0.74, but no time point met the prespecified 1-point minimal clinically important difference. 5
Evidence strength. The study is pragmatic and operationally relevant because the program used telehealth group visits and incorporated primary care clinicians. The trial is registered as ClinicalTrials.gov NCT04129450. 5
Clinical implication. The paper supports a scalable nonpharmacologic care model for chronic low back pain, but the effect size argues against overselling the intervention as a large pain-control advance. The read decision depends on whether the reader is optimizing population-level access to low-risk supportive care or looking for a clinically large individual-level treatment effect.
Bottom line for triage
If you open only one paper outside your specialty, start with the acetaminophen sibling-matched analysis because it changes how a common pregnancy-safety question can be framed at the bedside. If you follow pediatric endocrinology or genetics, the NEJM infigratinib trial is the cleanest phase 3 efficacy read. ReMIND is the most biologically ambitious paper, but it belongs in the early-phase research file until later comparative data arrive.
For implementation work, the TBI biomarker paper and OPTIMUM trial may be more immediately useful than their ranking suggests. One flags a subgroup risk for false reassurance in Alzheimer blood testing; the other defines the likely effect size of a scalable chronic-pain care model.
Cover image: image from Multi-antigen-targeting T cells in pediatric central nervous system tumors: a phase 1 trial.
参考来源
- 1Prenatal Acetaminophen (Paracetamol) Use and the Risk of Autism and/or Attention-Deficit/Hyperactivity Disorder Among Sibling-Matched Cohorts
- 2Phase 3 Trial of Oral Infigratinib in Children with Achondroplasia
- 3Multi-antigen-targeting T cells in pediatric central nervous system tumors: a phase 1 trial
- 4Prior Traumatic Brain Injury and Alzheimer Disease Blood Biomarkers
- 5Mindfulness-Based Group Medical Visits for Persons With Chronic Low Back Pain: A Randomized Clinical Trial
围绕这条内容继续补充观点或上下文。