2026/7/5 · 0:17
Wernicke's area: why language comprehension is not one spot
Wernicke's area began as the classic counterpart to Broca's area, but modern lesion mapping and neuroimaging show that language comprehension depends on a distributed network. This article follows the original 1874 aphasia model, the evidence that unsettled it, and the dual-stream view that replaced the old one-box map.

If you learned the old map of language, Wernicke's area was the neat counterpart to Broca's area: Broca spoke, Wernicke understood. That picture is memorable, and it is also too tidy. Modern evidence makes Wernicke's area look less like a comprehension center and more like one node in a left-hemisphere language network, especially tied to sound-based word forms and the interface between hearing, words, and speech production.
The original idea: a sensory language center
Carl Wernicke's 1874 monograph, Der aphasische Symptomencomplex, is the landmark source for the idea that language disorders could be divided by anatomy, not just by outward symptoms 1. Wernicke described patients whose speech was fluent but poorly understood, and he linked that pattern to posterior left temporal damage. The contrast with Broca's earlier cases was powerful: one frontal lesion pattern seemed to disrupt articulate speech, while a more posterior lesion pattern seemed to disrupt the interpretation of speech.
That is the birth of the textbook phrase "Wernicke's area." In many diagrams, it sits in the posterior superior temporal gyrus, close to auditory cortex. The classic story says that this region stores or analyzes the sound patterns of words. Damage it, and speech can remain effortless in rhythm and grammar while meaning falls apart.
The deeper contribution was not the exact borders of the area. It was the method: use selective breakdowns after brain injury to infer the parts of a mental system. If one patient can hear but cannot understand speech, and another can understand but cannot produce fluent speech, then language is unlikely to be one indivisible faculty.
Why the old box became unstable
The difficulty is that "Wernicke's area" came to mean several different things at once. Sometimes it meant the posterior superior temporal gyrus. Sometimes it included adjacent parietal cortex, such as the supramarginal or angular gyrus. Sometimes it meant the lesion region found in patients with Wernicke's aphasia. Sometimes it meant the functional machinery for language comprehension.
Those are not the same claim. An anatomical label asks, "Where is this patch of cortex?" A syndrome label asks, "What symptoms tend to appear after a lesion?" A functional claim asks, "What computation does this tissue perform?" Modern neuroscience has pressed hardest on the third claim.
Binder's open-access review makes the problem bluntly: the historically defined Wernicke area is usually placed around the lower posterior left sylvian fissure, but modern lesion and imaging evidence does not support treating that patch as the critical site for word or sentence comprehension 3. Instead, comprehension draws on a broader temporal, parietal, and frontal system.
This distinction matters because lesion syndromes are messy. A stroke rarely removes only the tidy region drawn in a textbook. It can damage cortex, underlying white matter, blood-supply territories, and neighboring regions. A patient with Wernicke's aphasia may therefore have a large lesion that includes posterior temporal cortex plus other language-relevant tissue. If we name the whole syndrome after one cortical patch, we risk mistaking a rough clinical landmark for a precise mechanism.
What lesion mapping changed
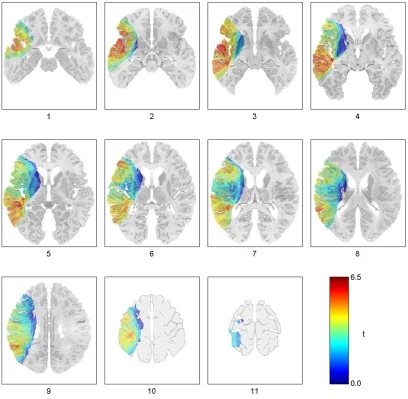
Large lesion studies let researchers ask a sharper question: across many patients, which damaged voxels best predict impaired comprehension? A voxel is a tiny 3D unit in a brain image. Voxel-based lesion-symptom mapping compares patients voxel by voxel, asking whether injury at each location is associated with a behavioral deficit.
Dronkers and colleagues studied 64 chronic left-hemisphere stroke patients on 11 receptive-language subtests. Patients heard sentences and chose the matching picture from a small array. The analysis linked comprehension performance to five left-hemisphere regions, including the posterior middle temporal gyrus, anterior superior temporal gyrus, superior temporal sulcus/angular gyrus region, mid-frontal cortex, and inferior frontal gyrus area 47. Lesions to the traditional Broca's and Wernicke's areas were not found to significantly alter comprehension on that measure 4.
That result does not mean the posterior temporal lobe is irrelevant. It means the old one-box explanation fails. Word-level and sentence-level comprehension lean on partly different regions, and the system includes long-range connections.
Turken and Dronkers pushed the point further by combining lesion results with diffusion tensor imaging, a method that estimates major white-matter pathways. Their paper describes language comprehension as a network architecture, with gray-matter regions connected by white-matter routes 5. For a reader, the important shift is simple: language comprehension is not just where neurons sit, but how regions communicate.
The modern replacement: streams and networks
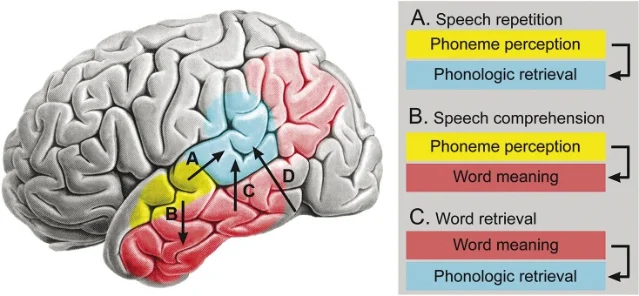
A useful replacement for the old box map is the dual-stream view of speech processing. Hickok and Poeppel argue that speech processing splits into two broad pathways. A ventral stream maps sound toward meaning. A dorsal stream links sound to articulatory and motor systems, helping with repetition, speech production, and short-term verbal memory 6.
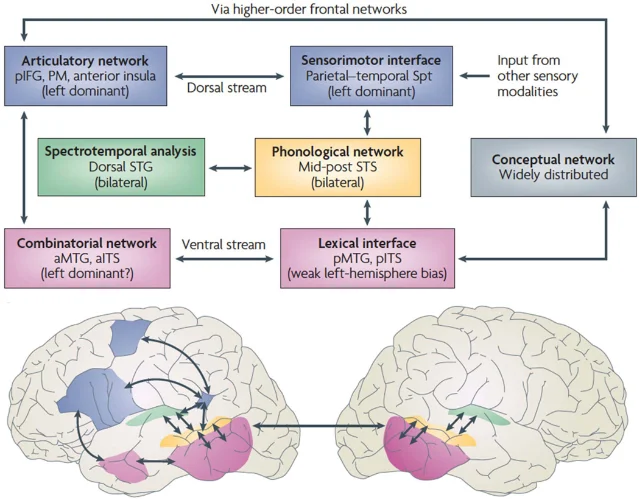
On this view, posterior superior temporal cortex is important, but it does not do all the work that the phrase "language comprehension center" suggests. Binder's later review states the revision even more strongly: the term Wernicke's area, if used at all, should not refer to a zone critical for speech comprehension. The region is better associated with retrieval of phonological forms, the mental sound patterns of words, which matter for speech output and short-term memory 7.
That claim helps explain why classical aphasia labels can still be clinically useful while being scientifically imperfect. A doctor may need a quick shorthand for a syndrome: fluent speech, poor comprehension, naming trouble, phonemic errors. A neuroscientist asking how the brain understands a sentence needs a more detailed model: auditory analysis, lexical access, semantic memory, syntax, working memory, attention, and motor-articulatory mapping.
What Wernicke's area teaches us now
The best way to keep Wernicke's area is as a historical doorway rather than a finished answer. It introduced three ideas that remain central.
First, language can break selectively. Aphasia showed that speech, comprehension, repetition, naming, and reading can dissociate. That still drives cognitive neuroscience: when a mental ability breaks in a patterned way, the pattern can reveal the architecture underneath.
Second, the brain's language system is left-lateralized for many people, but not locked into two isolated boxes. The left temporal lobe matters for mapping sound and meaning. Frontal and parietal regions matter too. White-matter pathways matter because they carry information between those regions.
Third, familiar names can outlive their original precision. "Wernicke's area" is convenient, but convenience can freeze a theory. A label that began as a clinical-anatomical hypothesis became a classroom map, then a target for modern evidence to refine.
For a non-specialist, the practical takeaway is this: understanding language is not like opening a dictionary in one cortical drawer. The brain has to transform air-pressure changes into phonemes, match phonemes to words, link words to concepts, combine them into sentence meaning, and coordinate those meanings with memory and action. Wernicke's area belongs in that chain, but it is not the whole chain.
Landmark paper
Carl Wernicke's 1874 monograph, Der aphasische Symptomencomplex: eine psychologische Studie auf anatomischer Basis, is the landmark source. The Wellcome Collection record identifies the work as an 1874, 72-page book published in Breslau by Max Cohn & Weigert and available online under a Public Domain Mark 1.
Course connection
This article connects directly to MIT 9.13 Lecture 18, "Language I," where Nancy Kanwisher frames the basic organization of language in the brain and the larger question of how language relates to thought 8. Wernicke's area is a good next step after Broca's area because it shows the same lesson from the opposite side: the classic lesion map was the beginning of the science, not the final wiring diagram.
参考来源
- 1Wellcome Collection: Der aphasische Symptomencomplex
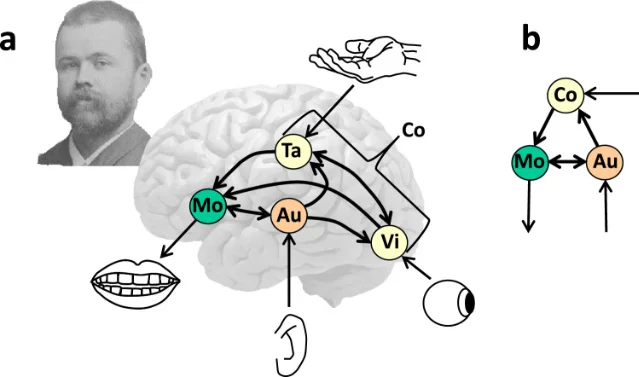
- 2Roelofs, 2024, Wernicke's functional neuroanatomy model of language turns 150
- 3Binder, 2015, The Wernicke area: Modern evidence and a reinterpretation
- 4Dronkers et al., 2004, Lesion analysis of the brain areas involved in language comprehension
- 5Turken and Dronkers, 2011, The Neural Architecture of the Language Comprehension Network
- 6Hickok and Poeppel, 2012, The cortical organization of speech processing
- 7Binder, 2017, Current Controversies on Wernicke's Area and its Role in Language
- 8MIT OpenCourseWare, 9.13 Lecture 18: Language I
更多来自该频道
相似内容
- 登录后可发表评论。