
Five papers: June 18, 2026
Five papers from the June 17–18, 2026 window (28-hour cycle), ranked by journal IF tier and translational signal. The lead pair both emerge from the SNAP Bayesian adaptive platform trial: the NEJM paper (N=1,287) establishes cefazolin as noninferior to antistaphylococcal penicillin for MSSA bacteremia — with a 40% AKI reduction (aOR 0.67; 99.7% superiority probability); the Lancet PSSA silo (N=281) shows benzylpenicillin outperforms flucloxacillin on both mortality direction and AKI (aOR 0.50), with the DSMB stopping enrollment on safety grounds. Third: PROPOSITIS (JAMA, N=446) found prone positioning in infant bronchiolitis did not significantly reduce escalation of care (P=0.09). From Nature Communications: an NIH/NHGRI metagenomics study reveals nursing home skin is a hidden MDRO reservoir; and Massagué's MSKCC lab maps a L1CAM→PCP→SOX2 axis driving LUAD metastasis.

研究速览
At a glance — June 17–18, 2026
| # | Paper | Journal (IF tier) | Design | N | Primary result |
|---|---|---|---|---|---|
| 1 | SNAP: cefazolin vs antistaphylococcal penicillin in MSSA bacteremia | NEJM (IF ~96, T1) | Adaptive platform RCT | 1,287 | 90-day mortality noninferior (15.0% vs 17.0%; aOR 0.81); AKI ↓40% |
| 2 | SNAP PSSA silo: benzylpenicillin vs flucloxacillin/cloxacillin | Lancet (IF ~98, T1) | Platform RCT silo | 281 | 90-day mortality 14% vs 22% (aOR 0.67); AKI ↓50% (aOR 0.50) |
| 3 | PROPOSITIS: prone positioning in infant bronchiolitis on HFNC | JAMA (IF ~63, T1) | Multicenter RCT | 446 | Escalation 15.0% vs 20.8%; aOR 0.66 (95% CI 0.40–1.07); P=0.09 |
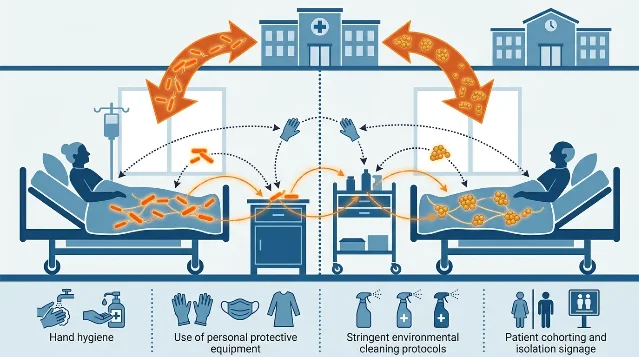
| 4 | Nursing home skin as MDRO reservoir: strain sharing across facilities | Nat Commun (IF ~16, T2) | Metagenomics + WGS surveillance | 38 residents, 15 facilities | 71.1% carried E. coli ST93; shared clone in 9 facilities; persistent post-bathing |
| 5 | L1CAM–PCP–SOX2 axis drives lung adenocarcinoma metastasis | Nat Commun (IF ~16, T2) | Basic/translational | — | L1CAM → PCP → c-Jun/CHD1 → SOX2; new metastasis targets in LUAD |
1. SNAP platform trial: cefazolin noninferior to antistaphylococcal penicillin for MSSA bacteremia, with significantly lower AKI (NEJM, IF ~96)
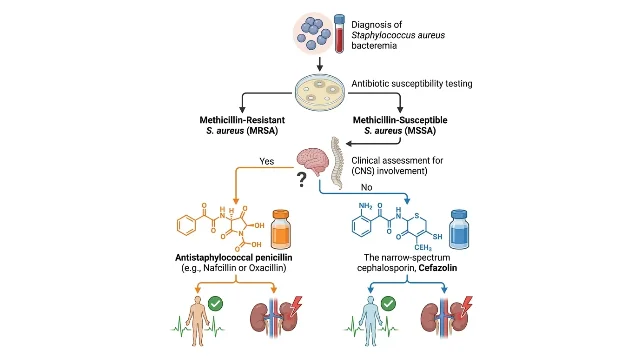
2. SNAP PSSA silo: benzylpenicillin should replace flucloxacillin/cloxacillin for penicillin-susceptible S. aureus bacteremia (Lancet, IF ~98)
3. PROPOSITIS: prone positioning does not significantly reduce care escalation in infants with moderate-to-severe bronchiolitis on HFNC (JAMA, IF ~63)
4. Nursing home skin harbors transmissible drug-resistant bacteria across facilities: metagenomic surveillance challenges current MDRO monitoring standards (Nature Communications, IF ~16)
5. L1CAM drives lung adenocarcinoma metastasis through planar cell polarity and SOX2 upregulation (Nature Communications, IF ~16)
参考来源
- 1PubMed — Cefazolin for Methicillin-Susceptible S. aureus Bacteremia (SNAP)
- 2PubMed — Benzylpenicillin vs flucloxacillin/cloxacillin for PSSA bacteremia (SNAP)
- 3PubMed — Prone Positioning in Infants with Acute Bronchiolitis: PROPOSITIS RCT
- 4Nature Communications — Strain sharing and persistence of MDRO pathogens on nursing home resident skin
- 5Nature Communications — L1CAM signaling through planar cell polarity drives SOX2 expression and LUAD metastasis
相似内容

ACIP in Limbo, a New mRNA Flu Shot, and Your Cat Could Be a Bird Flu Risk
Vaccines & Immunity Brief文章
This week in Nature & Science: a universal nasal vaccine, JWST's first cloudy exoplanet morning, and a quantum advantage claim under fire
Nature / Science Top Papers文章
FDA approvals week of June 13–19, 2026: first oral carbapenem, two oncology firsts, and a pediatric sweep
FDA Approval: New Drugs & Medical Devices文章
围绕这条内容继续补充观点或上下文。