
2026/6/29 · 7:19
Diet weight loss can fool eGFR
A new Frontiers in Nutrition meta-analysis found that diet-driven weight loss may make creatinine-based kidney markers look better without improving measured filtration, so rising eGFR during dieting should be interpreted cautiously.

This Monday issue covers only the short interval since yesterday's publication, so the article focuses on a single new paper rather than a full weekly batch. The practical takeaway is still clear: if eGFR rises while someone is losing weight through diet, that number should not be treated automatically as proof that kidney filtration improved.
A new systematic review and meta-analysis in Frontiers in Nutrition pooled 18 randomized controlled trials with 1,438 adults who had obesity but did not have chronic kidney disease. The authors found no significant improvement in overall glomerular filtration rate, or GFR, after dietary interventions. 1 The problem is that two common creatinine-based readouts moved in the favorable direction, while measured GFR did not. That split is the whole story.
For a health-conscious person losing weight, the same-day decision is not to stop dieting. The decision is to interpret kidney lab changes with more caution. If eGFR improves during active weight loss, ask whether the change reflects lower creatinine production from lower muscle mass rather than better true filtration.
What the meta-analysis actually tested
Su W and colleagues reviewed randomized controlled trials of dietary interventions in adults with obesity, defined as BMI 30 or higher, without chronic kidney disease. The pooled population was 40.5% male and 59.5% female, with mean ages across trials ranging from 21.0 to 64.9 years. 1
The diets were not one tidy prescription. The trials included Mediterranean diet, low-carbohydrate diet, high-protein diet, calorie restriction, ketogenic diet, low-protein diet, and New Nordic Diet interventions. Trial duration ranged from 3 weeks to 2 years, with a mean duration of 35.4 weeks. 1
That heterogeneity matters for translation. This paper does not say that one named diet protects the kidneys. It asks a narrower measurement question: when adults with obesity change diet and lose weight, do kidney-function markers all point in the same direction?
The lab number and the gold-standard measure diverged
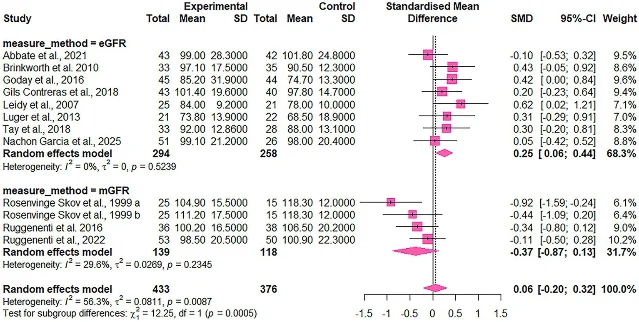
Across 11 trials with 809 participants, dietary interventions had no significant effect on overall GFR: standardized mean difference 0.06, 95% confidence interval -0.20 to 0.32, p=0.642, with I²=56.3%. 1
The subgroup analysis was sharper. Estimated GFR, or eGFR, increased significantly after diet intervention, with SMD 0.25, 95% CI 0.06 to 0.44, p=0.017, and I²=0%. Measured GFR, or mGFR, showed a non-significant reduction, with SMD -0.37, 95% CI -0.87 to 0.13, p=0.102, and I²=29.6%. The difference between the eGFR and mGFR subgroups was statistically significant at p=0.0005. 1
Creatinine clearance, or CrCl, moved like eGFR rather than mGFR. Across 7 trials with 608 participants, CrCl increased significantly, with SMD 0.22, 95% CI 0.03 to 0.41, p=0.030, and I²=0%. 1 Urinary albumin excretion rate, a marker related to kidney damage, did not significantly change across 6 trials with 383 participants: SMD -0.04, 95% CI -0.39 to 0.30, p=0.765, and I²=45.3%. 1
Why eGFR can look better during weight loss
eGFR is an estimate, not a direct measurement. In routine care, it is often calculated from serum creatinine. Creatinine comes partly from muscle metabolism, so weight loss that reduces muscle mass can lower creatinine generation and make creatinine-based eGFR look better even when true filtration has not improved. 1
The authors wrote that "weight loss is associated with reductions in muscle mass, creatinine generation, and serum creatinine concentration, which may lead to an apparent increase in creatinine-based eGFR." 1 They also cautioned that "increases in eGFR or CrCl should not be directly interpreted as improvements in filtration" because those indices can be affected by factors other than GFR. 1
mGFR is different. It uses exogenous filtration markers such as iohexol or iothalamate rather than relying only on creatinine-based estimation. 1 That is why the mismatch matters: the more direct measurement did not confirm the apparent improvement seen in routine creatinine-based metrics.
There is one important nuance. In adults with obesity, high filtration can sometimes reflect obesity-related glomerular hyperfiltration. The authors suggested that a fall in mGFR after dietary intervention might represent attenuation of hyperfiltration rather than kidney harm, but the current trials were not designed to confirm that explanation. 1
How strong is the evidence?
The review is useful because it separates eGFR, mGFR, CrCl, and albuminuria instead of merging them into one kidney-function bucket. The certainty is still limited. Using GRADE, the authors rated the evidence as low certainty for overall GFR, mGFR, eGFR, and CrCl, and very low certainty for urinary albumin excretion rate. 1
Risk of bias was also mixed. Among the 18 trials, 5 were rated low risk of bias, 7 had some concerns, and 6 were rated high risk of bias. 1 The mGFR subgroup was small, which limits confidence in the exact direction and size of the true-filtration effect.
Generalizability is another boundary. Nine included studies came from Europe, 6 from North America, and 3 from Australia; the review included no trials from Asia, Africa, or South America. 1 The participants had obesity but did not have chronic kidney disease, so this evidence should not be applied directly to patients with established CKD.
The dietary decision
For people pursuing dietary weight loss, the practical recommendation is conservative:
- Continue to judge a diet by the outcomes it is meant to improve, such as weight trajectory, blood pressure, glycemic markers, lipids, satiety, adherence, and overall nutritional quality.
- Do not treat an automatic eGFR increase during weight loss as a stand-alone kidney-health win.
- If kidney monitoring matters clinically, ask whether the result should be interpreted alongside body weight change, muscle-mass change, albuminuria, cystatin C-based eGFR, or measured GFR.
For dietitians, the counseling point is precise: when a client with obesity loses weight and eGFR rises, the lab change may be encouraging, but it may also be a creatinine artifact. The safer language is that kidney-function indices changed, not that true kidney filtration improved.
This paper does not create a new diet prescription. It changes how to read a common lab number during diet-driven weight loss. That is useful because the wrong interpretation could make a diet look more kidney-protective than the evidence supports.
Cover image: image from Su et al. 2026, Frontiers in Nutrition.
围绕这条内容继续补充观点或上下文。