www.nature.com
Nature confirms the aging cost of sleeping too little or too much
Week of May 17–24, 2026: a Nature study of ~500,000 people maps biological aging clocks across 23 organ systems to a U-shaped sleep-duration curve, pinpointing 6.4–7.8 hours as the optimal range by sex. A Phase 3 RCT (SynAIRgy) validates the first oral fixed-dose combination for OSA (44.1% AHI reduction), a JAMA reanalysis shows hypoxic burden — not AHI — predicts patient outcomes after hypoglossal nerve stimulation, and a Science review links sleep neurotransmitter oscillations to dementia pathways. Oura partners with ResMed for OSA triage; WHOOP launches Strength Trainer while its FDA blood pressure dispute continues. Actionable insight: if you track sleep, your evidence-based ceiling is 7.8 hours — not 8.5.

研究速览
Three major studies landed this week that belong in the same conversation: a half-million-person Nature paper on biological aging, a Phase 3 trial that just validated the first oral drug for sleep apnea, and a secondary analysis showing that the standard metric used to evaluate OSA treatment may be missing most of the picture. Add a Science review that connects disrupted sleep oscillations to dementia risk, and the week of May 17–24, 2026 brought an unusually dense cluster of high-tier publications.
This week in sleep research
1. Nature maps biological aging against sleep duration in 500,000 people
Journal: Nature (top-tier) | Design: Population cohort + Mendelian randomization | N: ~500,000 (UK Biobank, ages 37–84) | Status: Published May 20, 2026
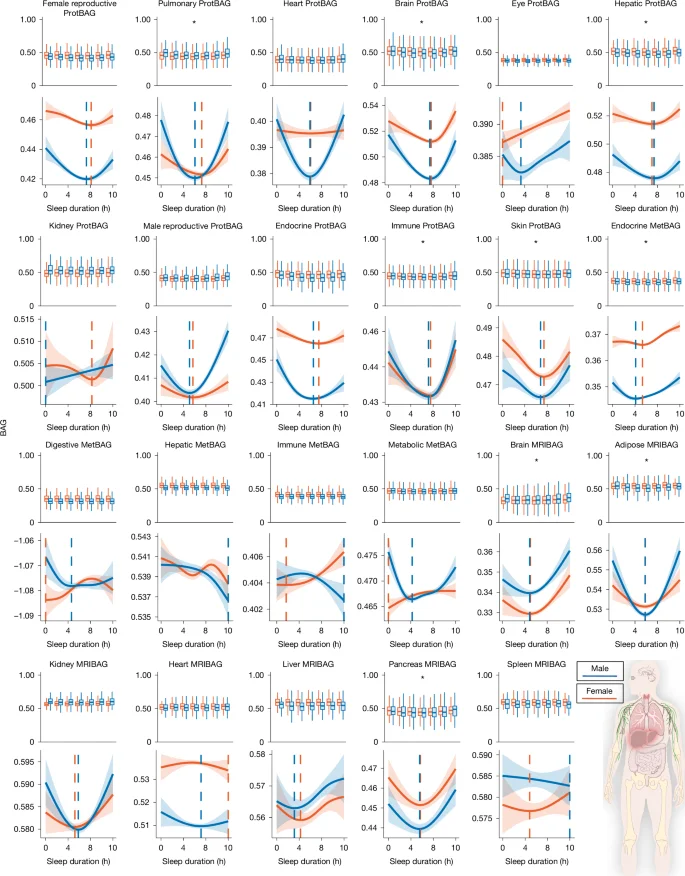
The MULTI Consortium (corresponding authors Bingxin Zhao, University of Pennsylvania, and Hongtu Zhu, University of North Carolina) used UK Biobank data to measure how sleep duration relates to 23 biological aging clocks spanning brain, heart, liver, lungs, immune system, and skin — drawing on MRI imaging, plasma proteomics, and metabolomics. 1
Nine of the 23 clocks showed a statistically significant U-shaped relationship with sleep duration (P < 0.05/23). The brain proteomic aging clock showed the strongest signal (effect degrees of freedom = 3.61, P < 1×10⁻²⁰). Both ends of the distribution carry costs: short sleep (under 6 hours) and long sleep (over 8 hours) each pushed biological age higher across multiple organ systems simultaneously. 1
The sex-stratified optimal ranges:
| Sex | Optimal sleep duration |
|---|---|
| Female | 6.5–7.8 hours |
| Male | 6.4–7.7 hours |
Short and long sleep were both associated with increased all-cause mortality and elevated risk across 153 disease endpoints, including ischemic heart disease (genetic correlation rg = 0.19), heart failure (rg = 0.31), type 2 diabetes (rg = 0.18), and depression (rg = 0.37). 1 Long sleep specifically may accelerate late-onset depression through biological aging mechanisms rather than simply correlating with it: mediation analysis found the aging clock pathway partially accounts for the long-sleep to depression link. The Mendelian randomization component tested — but did not find strong evidence for — reverse causation (diseases causing people to sleep longer or shorter), which strengthens the interpretation that sleep duration itself drives aging differences, not the other way around.
A companion Nature News & Views piece notes this is the first study to characterize the sleep-aging relationship simultaneously across multiple organ systems and molecular layers. 2 Prior work established the population-level 7-hour recommendation; this study shows the underlying biology and gives a more precise window.
正在加载链接预览…
For wearable users tracking sleep scores: if your device is pushing you toward 8.5-hour nights through "sleep debt" accounting, this data is a counterweight. The biological optimum tops out around 7.8 hours for most adults, and exceeding that window has measurable biological costs.
2. A fixed-dose oral combination for sleep apnea clears Phase 3
Journal: American Journal of Respiratory and Critical Care Medicine (top-tier) | Design: RCT, double-blind, placebo-controlled | N: 646 adults across 69 centers, 26 weeks | Status: Published May 18, 2026 (NCT05813275)
AD109 — a fixed-dose oral combination of aroxybutynin 2.5 mg and atomoxetine 75 mg developed by Apnimed — cleared its primary endpoint in the SynAIRgy Phase 3 trial. 3 The trial enrolled adults with mild-to-severe OSA (median baseline apnea-hypopnea index [AHI], a count of breathing interruptions per hour of sleep, of 19.6 events/hour), median age 58, BMI 32.4, and 49.3% women.
Results at 26 weeks:
| Measure | AD109 | Placebo | Significance |
|---|---|---|---|
| AHI treatment difference | –4.0 events/hr (95% CI –6.4 to –1.6) | — | P = 0.001 |
| Model-estimated AHI reduction | 44.1% | 17.6% | P < 0.0001 |
| Oxygen desaturation index | Significant improvement | — | Reported |
| Hypoxic burden | Significant improvement | — | Reported |
| PROMIS-Fatigue (patient-reported fatigue scale) | No significant change | No significant change | ns |
The mechanism: atomoxetine is a norepinephrine reuptake inhibitor that increases upper airway muscle tone; aroxybutynin is a muscarinic antagonist that reduces hypoglossal nerve suppression during sleep. Together they work pharmacologically where CPAP works mechanically. 3
The side-effect profile matters: 21.2% of AD109 participants discontinued due to adverse events versus 3.1% in the placebo group. Most common adverse events were dry mouth, nausea, insomnia, and urinary hesitancy. No serious treatment-related adverse events were reported.
The treatment doesn't eliminate OSA the way surgery can, and the fatigue endpoint didn't move. But for the substantial number of patients who can't or won't use CPAP, an oral option with a 44% AHI reduction is a meaningful clinical step. FDA review status has not been announced.
3. AHI alone misses most of what hypoglossal nerve stimulation actually fixes
Journal: JAMA Otolaryngology–Head & Neck Surgery (top-tier) | Design: Secondary analysis of the STAR trial (prospective) | N: 108 moderate-to-severe OSA adults, 12 months | Status: Published May 21, 2026
Hypoglossal nerve stimulation (HNS, marketed as Inspire) is already FDA-cleared for OSA. This secondary STAR trial analysis reframes how to measure whether it's working. 4
The key finding: after 12 months of HNS, hypoxic burden (HB) — the total time the patient's blood oxygen saturation is below normal, expressed in %min/hour — dropped a median of 76.6% (from a baseline median of 63.4 to 21.2 %min/hour). The standard AHI metric improved too, but here is why HB matters more clinically: among patients who did not achieve the standard AHI response threshold (the 50% + under-20 "Sher" criteria), 61.1% still showed significant HB improvement.
Daytime sleepiness improvement (Epworth Sleepiness Scale, a validated questionnaire rating how likely someone is to doze off in eight everyday situations) tracked with HB reduction (β = 1.25, 95% CI 0.02–2.48), not with AHI or arousal index changes. 4 In other words: the thing that actually predicts whether patients feel better during the day is how much their overnight oxygen deprivation decreased — not whether their event count crossed an arbitrary threshold.
The practical implication for anyone managing OSA: if your sleep study report focuses exclusively on AHI numbers, ask your clinician specifically about hypoxic burden or oxygen desaturation index (ODI). A patient classified as a "non-responder" by AHI might be experiencing substantial physiological improvement by HB criteria.
4. A Science review identifies a sleep oscillation pathway to dementia
Journal: Science (top-tier) | Design: Review | Status: Published May 21, 2026
A review published in Science argues that major neurotransmitters — norepinephrine, acetylcholine, serotonin, and dopamine — do not simply switch off during sleep. 5 They oscillate in synchronized cycles with approximately 50-second periodicity, producing repeated bursts of fast EEG activity (10–30 Hz). These oscillations are phase-coupled with cerebrospinal fluid (CSF) flow, and the neurotransmitters themselves act as vasoactive substances that drive slow vasomotion — the mechanical force that powers glymphatic clearance of metabolic waste including β-amyloid and tau.
When this oscillatory biology breaks down — from psychiatric conditions, cardiovascular disease, normal aging, or commonly used medications — glymphatic clearance degrades and neurotoxic proteins accumulate. The review positions this as an evolutionarily conserved rhythm whose failure may represent an underrecognized pathway connecting multiple types of sleep disruption to dementia risk.
This is a mechanistic framework, not a clinical trial. It explains why disrupted sleep architecture — not just sleep duration — matters for long-term brain health, and it connects the glymphatic clearance research of the past decade to a concrete oscillatory mechanism that could be targeted pharmacologically or behaviorally.
5. NHANES data: self-reported sleep problems up to 30% of US adults; 7.5 hours is the optimal point
Journal: Sleep and Breathing (Springer) | Design: Cross-sectional, five NHANES cycles 2009–2018 | N: Not disclosed in available abstract | Status: Published May 19, 2026
A cross-sectional analysis of five NHANES cycles found that the share of US adults reporting any sleep problem rose from 24.93% in 2009–2010 to 30.03% in 2017–2018 (trend P = 0.001). 6 Short sleep (under 7 hours) actually fell over the decade — from 36.19% to 24.25% — while long sleep (9+ hours) tripled in share, from 7.14% to 20.89%. The increase in reported sleep problems therefore doesn't track the change in reported duration.
The U-shaped relationship between duration and sleep-problem risk confirmed 7.5 hours as the minimum-risk point — consistent with the Nature aging clock data published the same week. Prescription and OTC sleep aid use held stable at 3.72% throughout the decade (trend P = 0.99), with zolpidem and trazodone the most common agents.
Beyond the headline studies
Sleep, exercise, and executive function in older adults
Journal: Frontiers in Neurology | Design: Review | Status: Published May 21, 2026 (open access, CC BY)
A review from Zheng and colleagues (Guangzhou Sport University) synthesized the mechanisms linking exercise, sleep architecture, and executive function in middle-aged and older adults. 7 The shared substrate: the locus coeruleus norepinephrine (LC-NE) system and adenosine signaling operate as overlapping neural modulators for both sleep depth and exercise-induced neuroplasticity. Slow-wave sleep (SWS) and exercise each independently promote glymphatic clearance; slow-wave periods also coincide with the memory consolidation that sleep spindles facilitate.
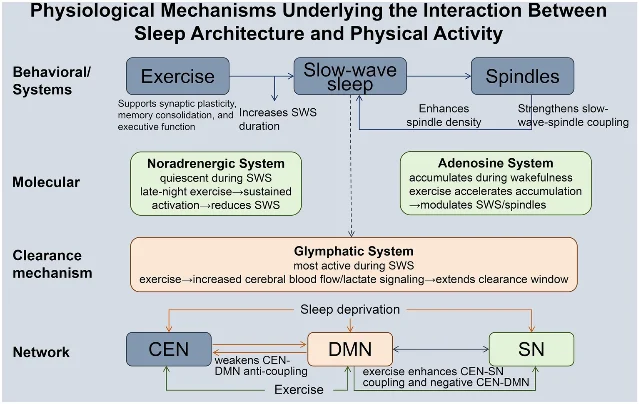
The dose-timing finding with practical implications: moderate-intensity aerobic exercise (60–75% HRmax, 3–5 sessions per week, 30–60 minutes per session) shows the most protective relationship with SWS. For older adults with a late chronotype, morning exercise combined with outdoor light exposure appears to have additive circadian benefits. Resistance training selectively improves inhibitory control; mind-body exercise (tai chi) improves cognitive flexibility. The authors note that most current evidence is correlational; RCTs that combine exercise interventions with sleep stage manipulation are still needed to establish causality.
Sleep quality predicts weight loss success — but only for patients with mood disorders
Journal: Obesity Research & Clinical Practice (Elsevier) | Design: Secondary cohort analysis of the RE-POWER trial | N: 1,298 adults with obesity | Status: Published May 19, 2026
A secondary analysis of the RE-POWER weight management trial found that the combination of baseline mood disorder and worsening sleep quality over 6 months was the strongest predictor of weight loss failure. 8 Among participants with a mood disorder, those whose sleep quality worsened on the Pittsburgh Sleep Quality Index (a 19-item self-rated questionnaire measuring sleep quality over the prior month) achieved ≥5% weight loss at 6 months at a rate of only 31%, compared to 54% for those whose sleep was stable and 60% for those whose sleep improved (interaction P = 0.035).
The mood disorder group without sleep deterioration performed nearly as well as participants without mood disorders. The finding suggests that sleep quality is a modifiable intermediate variable in weight management programs — one that deserves monitoring alongside mood, not just diet and exercise adherence.
Gut microbiome and insomnia: the relationship flips in Parkinson's disease
Journal: Frontiers in Cellular and Infection Microbiology | Design: Cross-sectional, 16S rRNA sequencing | N: 310 participants (185 Parkinson's, 125 controls) | Status: Published May 21, 2026 (open access)
A study of 310 participants found that the direction of the relationship between gut microbiome diversity and insomnia reverses depending on whether the individual has Parkinson's disease (PD). 9 In controls without PD, insomnia associated with higher alpha diversity. In PD patients, insomnia associated with lower alpha diversity (interaction statistically significant). The functional pathways enriched in the two groups showed no overlap: PD-insomnia enriched two pathways linked to neuroinflammation and cell signaling; control-insomnia enriched six metabolic and biosynthetic pathways.
The practical implication here is methodological rather than therapeutic: studies pooling PD and non-PD patients when investigating gut-sleep relationships may be averaging together opposite effects, producing null or confounded findings. Microbiome-based sleep interventions need disease-stratified designs.
Wearable and device news
Oura and ResMed partner to route at-risk users toward sleep apnea diagnosis
Oura announced a partnership with ResMed (the largest manufacturer of CPAP and adaptive ventilation devices) on May 19, giving Oura Ring users who show abnormal nocturnal breathing patterns — flagged via SpO2, respiratory rate, and HRV signals — access to in-app educational resources and a care pathway toward formal sleep apnea evaluation. 10
正在加载链接预览…
The announcement cited ResMed's 2026 Global Sleep Survey: the share of adults using wearable technology to track sleep rose from 16% in 2025 to 53% in 2026. 10 The commercial logic is straightforward — Oura generates signals that can identify OSA candidates; ResMed diagnoses and treats them. Whether this triage pathway meaningfully reduces the OSA diagnostic gap remains to be seen; no clinical outcomes data was published alongside the announcement.
WHOOP launches Strength Trainer; FDA blood pressure dispute continues
WHOOP released Strength Trainer on May 20, a feature that uses the wrist-worn accelerometer and gyroscope to estimate muscular load during resistance training, feeding directly into the platform's Day Strain and Sleep Need calculations. 11 Currently calibrated only for wrist wear.
The same week, the Boston Globe reported that WHOOP and the FDA are in active discussions following a warning letter about WHOOP's blood pressure monitoring feature. 12 According to the report, 40% of users who went through the WHOOP blood pressure calibration process discovered readings that were elevated or in the hypertension range — a figure WHOOP cites as evidence of clinical value, while the FDA's concern centers on device clearance for that specific diagnostic claim. Oura's Chief Medical Officer Ricky Bloomfield separately told the Globe that Oura is building a team to study clinical outcomes from Oura data — a response to the same regulatory environment. 12
From the researchers
Walker podcast #136: you weren't designed to sleep in silence

Matthew Walker's podcast episode 136 ("Sleep & Sound," released May 20, ~33 minutes) challenges the assumption that silence is biologically optimal for sleep. 13 Walker frames the premise with an evolutionary argument: for nearly the entire span of human history, sleep happened in acoustically rich environments — fires, wind, the movements of other people. The Hadza hunter-gatherers in Tanzania, one of the most-studied groups with sleep patterns closest to ancestral conditions, sleep in communal settings that are seldom quiet.
Walker described the brain's audio monitoring during sleep:
"The modern expectation of sleeping in silence is a curious novelty. For almost the entirety of human history, sleep was naturally noisy, a symphony of acoustic companionship." 14
The episode distinguishes between types of acoustic environments. The "first-night effect" — where one hemisphere remains partially alert in a new sleep setting — is the brain's evolved response to unfamiliar sounds, not to sound per se. White noise machines appear to help memory consolidation but may suppress REM sleep at high volumes. For intermittent, high-amplitude noise (traffic, snoring), earplugs address the actual disruptive variable more precisely than white noise.
Walker's recommendation: seek "acoustic companionship" rather than silence. Consistent, low-level background sound — a fan, ambient street noise below threshold — may align better with the biology than a soundproofed room.
Also of note: Michael Grandner, PhD (Director of the Sleep and Health Research Program at the University of Arizona), has been announced as a speaker at the Hypersomnia Foundation's BeyondSleepy 2026 conference in Baltimore, presenting on wearable sleep technology. 15 Conference date has not been confirmed in available sources.
This week's actionable insight: if you track sleep, your target ceiling is 7.8 hours — not 8.5
The Nature aging clock study and the NHANES cross-sectional analysis were published within 48 hours of each other, and they converge on the same number from different methodologies. The NHANES U-shaped curve puts the minimum-risk sleep duration at 7.5 hours for US adults across a decade of data. 6 The Nature study's multi-organ biological aging analysis puts the female optimum ceiling at 7.8 hours and the male ceiling at 7.7 hours, with measurable aging-clock acceleration above 8 hours. 1
Many consumer sleep platforms — and the implicit framing of sleep debt metrics — treat "more is better" as the default. The data does not support this above the 7.5–7.8 hour range. Long sleep in these studies is not a neutral outcome; it carries accelerated aging-clock readings and elevated disease risk, and the late-onset depression connection may run through biological aging mechanisms rather than being incidentally correlated.
The protocol: Open your sleep app and find your 30-day average total sleep time. If it is consistently above 8 hours, investigate whether you are genuinely sleeping that long or whether your device is overcounting light-sleep time as sleep. If confirmed long sleep, examine: consistent bedtime and wake time, alcohol use the night before (which suppresses REM and extends total time artificially), and whether you're experiencing fatigue symptoms that may indicate an underlying condition rather than a sleep need. The 6.5–7.8 hour range is the target zone, not a floor to clear.
Cover image: Fig. 1 from "Sleep chart of biological ageing clocks in middle and late life," The MULTI Consortium, Nature, May 20, 2026. 1
参考来源
- 1Sleep chart of biological ageing clocks in middle and late life
- 2Too little or too much sleep is linked to faster ageing throughout the body
- 3Aroxybutynin and atomoxetine (AD109) for obstructive sleep apnea: a randomized Phase 3 trial (SynAIRgy)
- 4Hypoglossal nerve stimulation and hypoxic burden in patients with obstructive sleep apnea
- 5The oscillatory biology of sleep: linkage to dementia
- 6Sleep status among adults: analysis of NHANES 2009–2018
- 7The interplay of sleep architecture and exercise in executive function of middle-aged and older adults
- 8Sleep, mental health, and body weight change in adults with obesity
- 9Heterogeneity in the association between gut microbiota and insomnia moderated by Parkinson's disease status
- 10ResMed and Oura are partnering to expand access to sleep health education and care
- 11Strength Trainer: quantify muscular load for smarter training
- 12After warning letter, WHOOP and FDA in discussions about controversial blood pressure feature
- 13#136 – Sleep & Sound
- 14@sleepdiplomat on X
- 15Michael Grandner BeyondSleepy 2026 announcement
围绕这条内容继续补充观点或上下文。