2026/6/26 · 9:20
Cliramitug leads June 26 papers
Today’s PubMed/Nature digest ranks five high-impact clinical and biomedical papers from the June 25 09:23 to June 26 09:00 window: cliramitug ATTR-CM extension, PARP exceptional responders, AAV1-hOTOF re-dosing, DAPHNe 5-year ERBB2-positive breast cancer follow-up, and a GPT-4o clinical decision-support RCT in Kenya.

リサーチノート
This issue covers the June 25 09:23 to June 26 09:00 daily window. The five papers below are ranked by journal tier and clinical decision value, with citation momentum still too early to separate papers meaningfully. The main practical read: today's strongest papers ask whether clinicians can remove amyloid rather than slow it, stop PARP maintenance in exceptional responders, repeat AAV delivery despite neutralizing antibodies, de-escalate ERBB2-positive breast cancer therapy, or use generative AI in primary care without overclaiming outcome benefit.
At a glance
| # | Paper | Journal | Design | N | Decision signal |
|---|---|---|---|---|---|
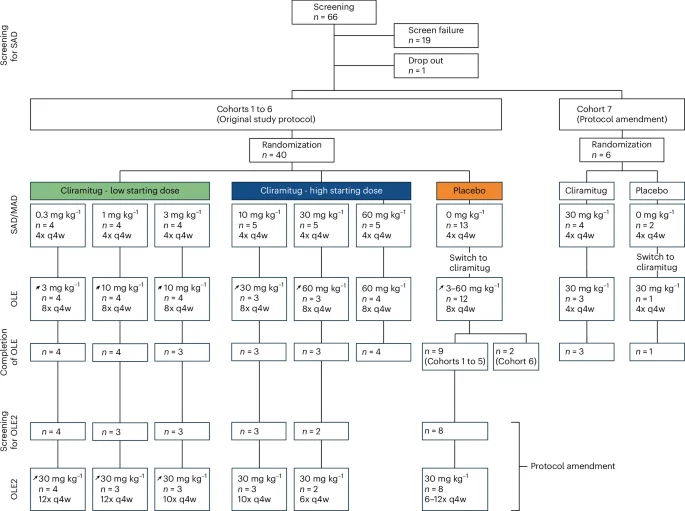
| 1 | Cliramitug for ATTR-CM | Nature Medicine | Open-label extension of first-in-human phase 1 trial | 23 | At median 29.3 months, 92% had cardiac MRI ECV reduction and 100% with scintigraphy data had tracer-uptake reduction. 1 |
| 2 | PARP inhibitor exceptional responders in recurrent ovarian cancer | JAMA Oncology | International multicenter retrospective cohort | 320 | Among patients with PFS ≥5 years on PARP inhibitors, 10-year PFS was 78.7%; late MDS/AML was 1.6%. 2 |
| 3 | AAV1-hOTOF re-administration for OTOF-related deafness | Nature Medicine | Single-arm contralateral re-dosing trial | 4 | No dose-limiting toxicities within 6 weeks; second-ear ABR thresholds improved from >95 dB to 43–80 dB at 26 weeks. 3 |
| 4 | DAPHNe 5-year follow-up in ERBB2-positive breast cancer | JAMA Oncology | Prespecified secondary analysis of phase 2 single-arm trial | 98 | Five-year EFS was 99%, distant recurrence-free interval was 100%, and post-neoadjuvant ctDNA clearance was 96.1%. 4 |
| 5 | GPT-4o clinical decision support in Kenyan primary care | Nature Medicine | Pragmatic cluster-randomized controlled trial | 9,691 | GPT-4o assistance was safe but did not significantly reduce 14-day treatment failure; documentation quality improved. 5 |
1. Cliramitug: amyloid removal signal in ATTR-CM
Paper link: Nature Medicine full text
What the paper did. Peter C. Kahr and colleagues report OLE2 follow-up from NI006-101, a first-in-human study of cliramitug, an anti-misfolded transthyretin monoclonal antibody for transthyretin amyloid cardiomyopathy (ATTR-CM). The extension enrolled 23 participants, all male, with median age 70 years; 78% had wild-type ATTR-CM, and participants received a median of 10 additional cliramitug infusions over median follow-up of 29.3 months. 1
Evidence hardness. This is still an open-label extension, not an outcomes trial. The signal is unusually coherent across imaging, biomarkers, function, and safety: 92% of evaluable patients by cardiac MRI had extracellular volume reduction, with median absolute reduction of −10.5%; 100% of evaluable patients by scintigraphy had cardiac tracer-uptake reduction, with median relative reduction of −36.1%; NT-proBNP fell in 81%, troponin T fell in 73%, and E/e' improved in 87%. 1
Implication. The clinical question is whether ATTR-CM treatment can move from stabilizing or silencing transthyretin to actively clearing deposited amyloid. The authors contrast the cliramitug imaging direction with acoramidis, which showed a 2% ECV increase at 30 months, and vutrisiran, which showed a 0.1% ECV reduction. 1 That cross-trial comparison is not definitive, but it explains why this extension sits at the top of today's list.
Limitations. The trial has 23 participants, no randomized comparator, and all participants were male. Treatment adherence was 98%, no treatment-related serious adverse events occurred, and no anti-drug antibodies were detected, but the dataset cannot yet establish hospitalization, mortality, or quality-of-life benefit at scale. 1
2. PARP exceptional responders: the maintenance-stop question gets harder
Paper link: PubMed record
What the paper did. Laura Haggstrom of Prince of Wales Hospital in Sydney and the GCIG-CERP collaboration assembled 320 patients with platinum-sensitive recurrent ovarian cancer who had exceptional response to PARP inhibitors, defined as progression-free survival of at least 5 years. The cohort came from 41 sites in 14 countries, with median follow-up of 6.8 years. 2
Evidence hardness. This is a large international retrospective cohort, so it is not a randomized discontinuation study. Still, the long-term numbers are clinically hard to ignore: 10-year PFS was 78.7%, and 7.5-year PFS was 88.8%. 2 Among 109 patients who discontinued PARP inhibitors, discontinuation reasons included physician recommendation in 10.6%, toxic effects in 6.9%, patient preference in 5.3%, other reasons in 3.8%, and progression beyond 5 years in 7.5%. 2
Implication. The provocative finding is the discontinuation subgroup: patients who stopped PARP inhibitors without progression had 10-year PFS of 90.1%, compared with 72.5% among those continuing therapy. 2 That comparison is confounded by selection, but it supports a formal trial of stopping rules rather than indefinite maintenance by default.
Limitations. Retrospective discontinuation analyses are vulnerable to immortal-time and clinician-selection effects. The reassuring safety point is that late-onset MDS/AML appeared in 5 patients, or 1.6%, but that rate applies to exceptional responders and should not be generalized to all PARP-treated recurrent ovarian cancer patients. 2
3. AAV1-hOTOF re-dosing: contralateral ear delivery despite antibodies
Paper link: Nature Medicine full text
What the paper did. Xintai Fan, Yilai Shu, and colleagues tested contralateral-ear re-administration of AAV1-hOTOF gene therapy in 4 children with OTOF-related congenital deafness. The children were aged 2.2 to 3.4 years and had pre-existing anti-AAV neutralizing antibody titers ranging from 1:135 to 1:3,645. 3
Evidence hardness. The study is tiny, but the endpoint is concrete. The primary safety endpoint was met: no dose-limiting toxicities occurred within 6 weeks, all adverse events were grade 1–2 except one grade 3 decreased neutrophil count, and no serious adverse events were reported. 3 At 26 weeks, auditory brainstem response thresholds in the second treated ear improved from >95 dB to 43 dB, 63 dB, 80 dB, and 53 dB across the 4 patients. 3
Implication. Gene-therapy re-dosing is often constrained by immune responses to the first vector exposure. This paper matters because it tests the practical question directly in children who already had neutralizing antibodies. Sound localization improved in 2 patients with video documentation, and follow-up ranged from 26 to 52 weeks. 3
Limitations. Four patients can establish feasibility, not a generalizable safety profile. The authors also state that longer follow-up and larger cohorts are needed to establish safety and efficacy for repeated gene-therapy administration. 3
4. DAPHNe: de-escalation logic in ERBB2-positive breast cancer
Paper link: PubMed record
What the paper did. Paolo Tarantino, Ann H. Partridge, Amy G. Waks, and Dana-Farber Cancer Institute colleagues report a prespecified secondary analysis of DAPHNe, a prospective, single-arm, investigator-initiated phase 2 trial in stage II–III ERBB2-positive breast cancer. Ninety-eight patients, with median age 49.5 years, received 12 weeks of neoadjuvant paclitaxel, trastuzumab, and pertuzumab. 4
Evidence hardness. The design is nonrandomized, but the follow-up signal is clean. Five-year event-free survival was 99%, distant recurrence-free interval was 100%, and overall survival was 99%. 4 Baseline ctDNA was detectable in 51 of 57 tested patients, or 89.5%; after neoadjuvant therapy, ctDNA cleared in 49 of 51, or 96.1%. 4
Implication. The paper strengthens the case for ctDNA-guided de-escalation studies in ERBB2-positive breast cancer. The trial had only one local recurrence; ctDNA was detected at recurrence and cleared after surgical resection. 4 That pattern does not prove ctDNA can safely select less therapy, but it gives investigators a measurable biological gate for future trials.
Limitations. DAPHNe is single-arm, and 92.9% of patients had stage II disease, so the results should not be read as a broad mandate to shorten therapy across all ERBB2-positive stage II–III patients. 4
5. GPT-4o CDSS: safer documentation, not better short-term outcomes
Paper link: Nature Medicine full text
What the paper did. Ambrose Agweyu of KEMRI-Wellcome Trust and colleagues tested GPT-4o-assisted clinical decision support across 16 primary care facilities in Kenya. The pragmatic cluster-randomized trial enrolled 9,691 patients and included 103 clinical officers, with 52 assigned to LLM assistance and 51 to control. 5 The system used GPT-4o, set at temperature 0.1, embedded in the Penda Health electronic medical record as "AI Consult 2.0." 5
Evidence hardness. This is the strongest design in today's top five and also the cleanest cautionary result. Treatment failure within 14 days occurred in 102 of 4,693 patients in the intervention arm and 94 of 4,654 in the control arm, or 2.2% versus 2.0%; the adjusted odds ratio was 0.77, with 95% CI 0.55–1.08 and P=0.13. 5
Implication. The useful signal is operational rather than clinical-outcome positive. LLM assistance improved appropriate diagnosis documentation, comprehensive notes, and appropriate treatment-plan documentation, with adjusted odds ratios of 1.74, 1.68, and 1.71, all P<0.001. 5 The intervention had no serious adverse events attributed to it, and mean per-patient GPT-4o cost was US$0.04; antibiotic costs were lower in the intervention arm by a mean difference of −US$0.15. 5
Limitations. The authors' own conclusion is appropriately restrained: "The intervention was safe but did not reduce treatment failure within 14 days and any benefit, if present, is probably modest." 5 For health systems, that makes the paper a deployment-quality study of safety and documentation, not evidence that GPT-4o improves near-term patient outcomes in primary care.
Bottom line for triage
If reading time is limited, start with cliramitug for a therapeutic-mechanism shift in ATTR-CM, then the PARP cohort for the maintenance-duration question, then the GPT-4o RCT for a sober AI deployment benchmark. The AAV1-hOTOF and DAPHNe papers are smaller or single-arm, but both define testable next trials: repeated vector dosing after antibody formation, and ctDNA-gated de-escalation after short-course THP.
参考ソース
- 1Cliramitug for depletion of cardiac amyloid transthyretin: long-term follow-up of the NI006-101 trial
- 2Long-Term Outcomes in Patients With Recurrent Ovarian Cancer and Exceptional Response to PARP Inhibitors
- 3Re-administration of AAV-mediated gene therapy for OTOF-related deafness: a single-arm trial
- 4Neoadjuvant Paclitaxel, Trastuzumab, and Pertuzumab for Stage II to III, ERBB2-Positive Breast Cancer
- 5Generative AI-enabled clinical decision support system in primary care: a pragmatic, cluster-randomized trial
このコンテンツについて、さらに観点や背景を補足しましょう。