
2026/6/22 · 9:23
Diet and Exercise Beat Metformin Over 20 Years — Plus: Fruit Juice, Fitness Trackers, and New Liver Transplant Guidelines
A 20-year NIH study finds lifestyle change cuts multimorbidity risk 21–25% in prediabetes — metformin doesn't. Plus: the FDA's first T1D disease-modifier for kids, a fitness tracker meta-analysis, and the first liver transplant guideline update since 2013.
Twenty years of data landed in a single study this week — and the headline is simpler than most medical news: if you have prediabetes, the most powerful thing you can do is eat better and move more. No prescription required. That finding anchors a week that also brought a milestone for children with type 1 diabetes, genuinely useful news for heart patients who own fitness trackers, and a set of liver transplant guidelines that should change how every transplant patient's long-term care is managed.
Here's what changed, why it matters, and what to bring to your next appointment.
Diabetes: the strongest long-term evidence yet for lifestyle change
A 20-year study settles the diet-and-exercise debate
The Diabetes Prevention Program (DPP) and its follow-up study (DPPOS) have tracked people with prediabetes — elevated blood sugar that isn't yet diabetes — since the late 1990s. This week, researchers published the 20-year results in JAMA, and the numbers are striking. 1
Among 1,173 Medicare-eligible participants who were followed through 2021, 85% had developed at least two chronic conditions by the study's end — a reminder of how common multimorbidity (having multiple diseases at the same time) is among older Americans. But the participants who had been assigned to an intensive lifestyle program were 21% less likely to develop two chronic conditions and 25% less likely to develop three, compared to the placebo group. 1
The lifestyle program was not exotic: 16 individual sessions over the first year focusing on reducing calories and fat, reaching 150 minutes of moderate exercise per week, and losing at least 7% of body weight, followed by monthly group sessions. The benefits held even when diabetes itself was excluded from the count of chronic conditions — meaning the program helped prevent other diseases, not just diabetes.
Metformin, the diabetes medication that was also tested in DPP, showed no statistically significant reduction in multimorbidity risk at 20 years. That doesn't make metformin useless — it has real benefits for blood sugar control — but it does reinforce that lifestyle change does something medication alone cannot.
Griffin P. Rodgers, MD, director of the NIH's National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), put it plainly: "Lifestyle programs focused on diet and exercise may persistently lower the risk of developing multiple chronic conditions, beyond diabetes." 1
<StatsDisplay title="NIH DPP/DPPOS: 20-year lifestyle intervention results" description="Among 1,173 Medicare-eligible adults with prediabetes, followed through 2021. Lifestyle program: 150+ min exercise/week, 7% weight loss goal, reduced-calorie diet. 1" stats={[{"key": "multi2", "label": "Lower risk of developing 2+ chronic conditions (lifestyle vs placebo)", "value": "−21%", "format": {"kind": "text"}}, {"key": "multi3", "label": "Lower risk of developing 3+ chronic conditions (lifestyle vs placebo)", "value": "−25%", "format": {"kind": "text"}}, {"key": "met", "label": "Multimorbidity reduction — metformin vs placebo", "value": "Not significant", "format": {"kind": "text"}}, {"key": "prev", "label": "Participants with 2+ chronic conditions by study end", "value": "85%", "format": {"kind": "text"}}]} />
Ask your doctor: "I have prediabetes — am I enrolled in or eligible for a National Diabetes Prevention Program? What's the closest CDC-recognized lifestyle program to me?"
The CDC-recognized version of the DPP is available in person and online across the US. Insurance coverage has expanded significantly, including Medicare. A simple Google search for "CDC National Diabetes Prevention Program near me" will find options.
FDA approves first treatment to slow early-stage type 1 diabetes in children
On June 12, the FDA granted accelerated approval to Tzield (teplizumab) for a new use: delaying the loss of insulin-producing capacity in children ages 8 to 17 who have just been diagnosed with Stage 3 type 1 diabetes (T1D). 2
To understand why this matters, a quick translation: type 1 diabetes is an autoimmune disease where the immune system destroys beta cells — the cells in the pancreas that make insulin. "Stage 3" means symptoms have appeared and insulin therapy has begun. Before Tzield, there was nothing available to slow that destruction once it started. Tzield works by partially dampening the immune attack.
Tzield was previously approved only for Stage 2 T1D (before symptoms appear) to delay progression to Stage 3. This new approval extends its use to children who have just crossed that threshold. The approval used a surrogate endpoint — a lab measure called C-peptide that reflects how much insulin the pancreas can still produce — and a post-market confirmatory trial is ongoing. 2
Mahtab Niyyati, MD, of the FDA's Center for Drug Evaluation and Research, said the approval "provides a chance for pediatric patients with recently diagnosed Stage 3 type 1 diabetes to alter the course of their disease." 2
Important caveats: Tzield carries a black box warning for serious viral reactivation (Epstein-Barr virus and CMV), and common side effects include vomiting, rash, elevated liver enzymes, and low white blood cell counts. It is given as an intravenous infusion over a 12-day course. It is not a cure — it slows progression — but for families navigating a new T1D diagnosis, it is the first approved tool to do that.
Ask your doctor: "My child was just diagnosed with Stage 3 type 1 diabetes — are they a candidate for Tzield? What does the infusion schedule look like, and what monitoring would be needed?"
For families in Louisiana: two pieces of good news
Louisiana Governor Jeff Landry signed Senate Bill 433, expanding Medicaid coverage of obesity medications in a state where about 39% of adults live with obesity. 3 Separately, the Louisiana House passed House Resolution 267, commissioning a comprehensive study of diabetes-related amputations in the state, with the goal of reducing them. 4
Both moves matter in a state that consistently ranks among the worst in the nation for diabetes-related complications. If you or a family member is on Louisiana Medicaid and has been told your weight-loss medication isn't covered, it's worth calling your plan again — coverage may have changed.
Cardiovascular: what you ate as a kid still matters, and your fitness tracker is doing more than you think
A 25-year study traces childhood drinks to adult blood pressure
Here's a finding that parents and grandparents will want to know — and that adults managing high blood pressure will want to bring to their next visit.

A study of 25,749 people, followed for up to 25 years from childhood through their mid-30s, found that drinking two or more sugary beverages per day as a child — soda, sports drinks, punch, sweetened iced tea — was linked to a 52% higher risk of developing high blood pressure as an adult, compared to children who drank fewer than three servings per week. The study was published in Circulation, the American Heart Association's (AHA) flagship journal. 5
The findings on fruit juice surprised even the researchers: drinking 1.5 or more servings of 100% fruit juice per day in childhood was linked to a 35% higher risk of high blood pressure. Orange juice specifically: 20% higher risk per daily serving. 5
The good news is that substitution works. Replacing one daily serving of sugary beverages with whole fruit was associated with a 22% lower risk of high blood pressure. Replacing fruit juice with whole fruit: 19% lower risk. Replacing sugary drinks with milk or water: up to 13% lower risk. 5
Amit Khera, MD (UT Southwestern, AHA volunteer expert) noted the key nuance: "There has been a misconception that fructose is harmful regardless of the source, and that fruit juices are beneficial for health. This study demonstrates that neither seems to be correct." 5 Whole fruit, where the sugar comes packaged with fiber, behaves differently in the body than juice, where it doesn't.
A note on scope: the study population was about 96% non-Hispanic white, and the authors specifically noted that the findings may be even more relevant for Black and Hispanic communities, where sugary drink consumption tends to be higher and hypertension rates are disproportionately elevated.
Ask your doctor: "Given my blood pressure history, should I be actively cutting back on even 100% fruit juice? What would you recommend as a replacement?"
Your fitness tracker is working — even if it doesn't feel like it
If you have heart disease and own a fitness tracker or use a smartphone health app, a new meta-analysis gives you a reason to keep using it.
Researchers analyzed 14 clinical trials involving 1,057 people with cardiovascular disease (CVD), all of whom used either wearable fitness trackers or smartphone apps to manage their physical activity. The result, published in the Journal of the American Heart Association: people using digital tools walked nearly 1,100 more steps per day and engaged in about 4 more minutes of moderate-to-vigorous exercise daily than those not using the tools. 6
The tools varied widely — some used gamification, some used coaching, some used simple step counters — but the benefits showed up regardless of design. They worked by using basic behavior-change principles: tracking progress, setting goals, and giving feedback.
Lead author Ajith Vemuri, PhD (Penn State Health) framed why this matters beyond gym memberships: "Many people with cardiovascular disease can't participate in traditional cardiac rehabilitation programs because of time, distance, or financial barriers." Smartphones and wearables, he noted, are already in people's pockets — "when effective, they can support routine care and reach a much wider population." 6
Damon L. Swift, PhD (University of Virginia, past chair of the AHA's Lifestyle Physical Activity Committee) added a concrete benchmark: "There is a reduced risk of death for even getting up to about 7,000 steps per day." 6 The meta-analysis didn't show significant improvements in peak cardiorespiratory fitness (VO2 max) or walking distance — longer studies are needed to confirm lasting fitness gains — but for day-to-day movement, the effect was consistent.

Ask your doctor: "Can you recommend a specific app or fitness tracker setup for someone with my heart condition? Should I aim for a particular step count, and is there a level where I should slow down?"
Heart failure care in older adults: a scientific statement flags a persistent gap
A new AHA scientific statement published in Circulation focuses on heart failure (HF) care in adults 65 and older — and the core finding is one patients and their families should know about: guideline-directed medical therapy (GDMT) for heart failure remains underused in older adults, even though clinical trials consistently show it helps them. 7
GDMT refers to the combination of medications proven by large clinical trials to reduce hospitalizations and death from heart failure — things like ACE inhibitors or ARBs, beta-blockers, and, more recently, SGLT2 inhibitors (like empagliflozin/Jardiance). Older patients with multiple conditions, frailty, or complex medication lists are often not started on these treatments or have them held back.
The statement calls for a domain management framework — a structured approach that evaluates not just cardiac function but also cognitive status, physical function, and social circumstances before making treatment decisions. It also explicitly recommends considering deprescribing: at every visit, ask whether any medications no longer align with the patient's goals.
For families: if an older parent or loved one has heart failure and seems to be on fewer medications than expected, or has never had a conversation about advance care planning, this statement signals that those conversations are now formally recommended as part of standard care. 7
Ask your doctor: "Is my heart failure treatment fully aligned with current guidelines? Is there anything I'm not on that might help — and are there any medications I might be able to stop?"
Liver disease: major new guidelines and a smartphone app that cuts hospitalizations in half
Two landmark liver transplant guidelines published
The American Association for the Study of Liver Diseases (AASLD) and the American Society of Transplantation (AST) published a comprehensive update to their adult liver transplant guidelines this month — the first major revision since 2013. The candidate evaluation guideline was published in Hepatology (June 2026). 8
For patients and families navigating serious liver disease, one of the most important things the guideline clarifies is when to ask for a transplant referral. The guidelines specify five types of events that should trigger immediate evaluation at a transplant center:
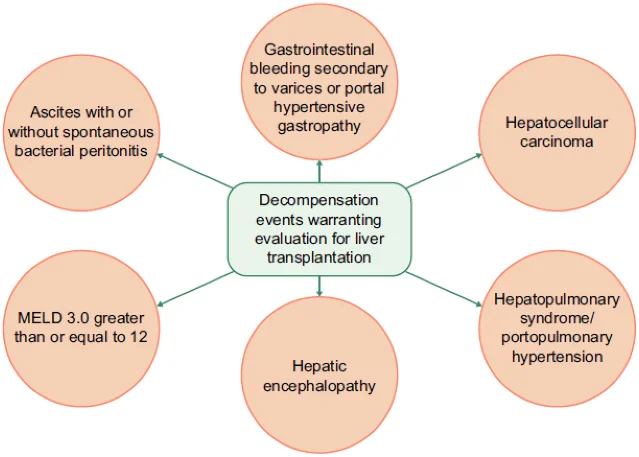
If any of these has occurred, the guideline is clear: "Liver transplant is a lifesaving procedure that should be offered to selected patients with clear indications and a reasonable prospect of benefit." 8 These are not situations to wait on.
A companion guideline covering long-term management after liver transplant — covering 87 recommendations across nine areas — was summarized this week in ACG Evidence-Based GI. 9 Key practical updates for transplant recipients:
- Annual metabolic screening — blood pressure, blood sugar, cholesterol, and weight — is recommended for all adult transplant recipients, because metabolic syndrome affects more than half of liver transplant patients and new cases develop in nearly a quarter of recipients within 15 months of transplant. 9
- For transplant recipients who develop diabetes or obesity, GLP-1 receptor agonists (the same class as semaglutide/Ozempic and tirzepatide/Mounjaro) are now recommended as first-line treatment for high-cardiovascular-risk patients — a meaningful shift from the standard immunosuppression-era diabetes management approach. 9
- Bone density scanning (DXA) at 6 months post-transplant, annual skin cancer checks, and colonoscopy as the preferred colorectal cancer screening method are all included. 9
- For patients of reproductive age: the guideline strongly recommends delaying pregnancy until at least 1 year post-transplant with at least 6 months of stable graft function. 9
Also published this week: new pediatric liver transplant guidelines from AASLD, the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition (NASPGHAN), and AST — covering both candidate evaluation and post-transplant management for children, all the way through the transition to adult care. 10
Ask your doctor (or your transplant team): "Has my care been updated to reflect the 2026 AASLD guidelines? Am I getting the annual metabolic screening that's now recommended? Is my diabetes or weight managed with the most current medications?"
A smartphone app cut cirrhosis hospitalizations nearly in half — a randomized trial
For people living with cirrhosis (scarring of the liver) and their caregivers, a well-designed study published in Hepatology this week offers genuinely encouraging news.
The HEROIC trial — a randomized study at three major medical centers (VCU Medical Center, Richmond VA Medical Center, and Mayo Clinic Rochester) — enrolled 232 cirrhosis patients and 232 of their caregivers between 2018 and 2024. 11 Half used the Patient Buddy App (tracking medication adherence, bowel habits, and symptoms) plus EncephalApp (a cognitive test for detecting early hepatic encephalopathy — the liver-related confusion that is the most common reason for hospitalization). The other half received standard care.
The result: within 30 days of hospital discharge, 10.3% of app users were readmitted for a preventable reason, versus 19.8% in the standard care group — nearly half as many. Overall 30-day readmission rates fell from 48% to 30%. 11
The app generated 1,660 alerts during the study. Many triggered real clinical actions: lactulose (a common bowel medication for encephalopathy) was adjusted in 62 cases, emergency outpatient visits were arranged in 35 cases, and drainage procedures for abdominal fluid were scheduled in 25 cases.
Senior author Jasmohan Bajaj, MD (VCU Medical Center), put it plainly: "Readmissions in cirrhosis patients are common and expensive. Reducing unnecessary and preventable readmissions is a major goal." 11 He also noted that hepatic encephalopathy "continues to be a major driver of these readmissions" — and that the app's cognitive tracking component was able to flag early signs before they escalated to a hospital visit.
The Patient Buddy App is not yet commercially available in the same form as studied, but the HEROIC trial results support asking your liver team whether any symptom-tracking tools are available to you.
Ask your doctor: "Are there symptom-monitoring apps or tools you'd recommend for managing my cirrhosis at home between appointments? What warning signs should trigger a call to your office or a trip to the ER?"
If you have type 2 diabetes and fatty liver: new evidence that GLP-1 medications protect the liver
A retrospective study using the All of Us Research Program — a large NIH database of US health records — examined 4,220 patients with both fatty liver disease (MASLD — metabolic dysfunction-associated steatotic liver disease) and type 2 diabetes. Half were taking GLP-1 receptor agonists (the medication class that includes semaglutide and tirzepatide); half were not. 12
Over a median follow-up of 2.7 years, the GLP-1 group developed cirrhosis, liver failure, liver cancer, or needed liver transplantation at a rate of 13.5 per 1,000 person-years — compared to 21.9 per 1,000 in the non-GLP-1 group. That works out to a 38% relative risk reduction (hazard ratio 0.62, 95% CI 0.46–0.83). The benefit was primarily driven by fewer cases of cirrhosis, and it held across subgroups defined by baseline liver fibrosis scores and BMI. 12
This is observational data — not a randomized trial — so it can't prove causation. But the finding complements existing clinical trial evidence and is consistent with what these medications are known to do: reduce liver fat, lower inflammation, and drive weight loss, all of which are protective for the liver.
Ask your doctor: "I have both type 2 diabetes and fatty liver — would a GLP-1 medication make sense for me? What's the evidence for liver benefit specifically?"
Good news for people with type 2 diabetes who get annual fibrosis screening
One more piece for patients with both type 2 diabetes and fatty liver disease: a prospective study at UC San Diego's MASLD Research Center found that repeating a non-invasive liver fibrosis assessment every two to three years — using the standard AGA clinical care pathway — cut the false-negative rate from 7% to 3%. 13
In plain English: the first screening misses some cases of significant liver scarring. Running the same panel two to three years later catches most of those missed cases, without overwhelming liver specialists with unnecessary referrals. Of 209 adults ages 50–79 with T2D who had two assessments over two years, 88.3% who were low-risk at baseline remained low-risk — so the repeat testing is not creating false alarms. 13
Lead researcher Veeral Ajmera, MD, summarized it concisely: "Serial reassessment works and the AGA Clinical Care Pathway is not meant to be applied once. Its accuracy improves when repeated at the recommended interval." 13
The standard pathway uses a blood test called FIB-4 — calculated from your ALT, AST, age, and platelet count, all available from a routine blood panel — to estimate whether significant liver fibrosis is present.
Ask your doctor: "I have type 2 diabetes — have I had a FIB-4 calculated recently? If it was done two or more years ago, should we repeat it?"
This week's "Ask Your Doctor" summary
The following questions capture the most actionable items from this week's updates. Bring the ones that apply to your situation to your next appointment.
| Who this is for | The question to ask |
|---|---|
| Adults with prediabetes | "Am I eligible for a National Diabetes Prevention Program lifestyle intervention near me?" |
| Parents of a child newly diagnosed with Stage 3 T1D | "Is my child a candidate for Tzield (teplizumab)?" |
| Louisiana Medicaid enrollees with obesity | "Does my plan now cover GLP-1 or other obesity medications under SB 433?" |
| Anyone with high blood pressure or a family history of it | "Should I cut back on fruit juice, not just soda?" |
| People with heart disease who own a fitness tracker | "What step count should I be aiming for, and are there any activities I should avoid?" |
| Older adults with heart failure | "Is my treatment fully aligned with current guidelines — and is there anything I'm not on that might help?" |
| Liver transplant recipients | "Has my post-transplant care been updated to the 2026 AASLD recommendations? Am I due for metabolic screening?" |
| People with cirrhosis | "Are there symptom-tracking apps you'd recommend for managing my condition at home?" |
| People with both T2D and fatty liver disease | "Would a GLP-1 medication benefit my liver specifically? When did I last have a FIB-4?" |
Coverage window: June 15–22, 2026. This digest summarizes clinically significant research and guideline updates published during that period. It is a starting point for conversations with your healthcare provider, not a substitute for individual medical advice.
参考ソース
- 1NIH: Lifestyle intervention lowered risk of developing multiple chronic conditions in adults with prediabetes
- 2FDA: FDA approves new indication for Tzield for certain pediatric patients with Stage 3 Type 1 Diabetes
- 3ADA: American Diabetes Association applauds Governor Landry on passage of Senate Bill 433
- 4ADA: ADA applauds Louisiana lawmakers for advancing diabetes-related amputation prevention through House Resolution 267
- 5American Heart Association: Does drinking juice, soda during childhood increase the risk of high blood pressure?
- 6American Heart Association: Smartphone apps, wearable trackers helped people with heart disease boost physical activity
- 7AHA Professional Heart Daily: Strategies for optimizing heart failure care in older adults
- 8PubMed/Hepatology: AASLD AST Practice Guideline on adult liver transplantation: Candidate evaluation
- 9ACG Evidence-Based GI: Beyond graft survival — a practical guide to long-term care after liver transplantation
- 10AASLD: New guidelines advance pediatric liver transplant care
- 11AGA GI & Hepatology News: Smartphone monitoring halves avoidable cirrhosis readmissions in randomized trial
- 12Gastroenterology Advisor: GLP-1 RAs reduce risk for hepatic complications in MASLD and T2D
- 13AGA GI & Hepatology News: Repeat fibrosis screening more than halves missed cases in type 2 diabetes



このコンテンツについて、さらに観点や背景を補足しましょう。