
2026/6/22 · 10:27
mRNA flu shot wins 9-0 — and August 5 is the date your family needs to know
The FDA's expert advisory panel voted unanimously on June 18 — twice, 9-0 — to recommend Moderna's first mRNA flu vaccine MFLUSIVA for adults 50 and older, setting an August 5 approval deadline that could put it in pharmacies this fall. But a court injunction keeps the CDC's ACIP committee frozen, leaving insurance coverage uncertain even if FDA approves. Measles hit 2,104 confirmed cases this week and is 184 short of the 2025 annual record; FluView confirms flu is at its summer floor with 182 pediatric deaths for the season; and Iowa families have nine days before a new law removes minors' ability to self-consent for HPV and hepatitis B vaccines.

A unanimous FDA expert panel vote, a coverage question that depends on a frozen committee, and a measles count that is 184 cases from a historic record. Here is where everything stands as of June 22.
FDA panel votes 9-0: Moderna's mRNA flu vaccine clears its biggest hurdle
On June 18, the FDA's Vaccines and Related Biological Products Advisory Committee (VRBPAC) — the independent expert group that evaluates new vaccine applications before the FDA makes a final ruling — voted unanimously on two separate questions about Moderna's MFLUSIVA (mRNA-1010), the first mRNA-based seasonal flu vaccine ever reviewed by this body in the United States. 1
- Adults 50–64: Do the benefits of MFLUSIVA outweigh its risks? → 9-0 Yes (standard approval pathway) 1
- Adults 65 and older: Same question? → 9-0 Yes (accelerated approval pathway, with a large confirmatory study required after approval) 2
The VRBPAC had not reviewed a new vaccine application since May 2023 (Pfizer's RSV vaccine), making this the first panel of its kind in over three years. The meeting ran about 6.5 hours. 3
コンテンツカードを読み込んでいます…
The PDUFA date — August 5, 2026 — is the FDA's self-imposed deadline to issue a final approval decision. If the FDA approves MFLUSIVA by that date, and if the CDC's advisory committee (more on its frozen state in Section 3) issues a timely recommendation, the vaccine could reach pharmacy shelves before the 2026–2027 flu season typically begins in September–October. 4
The road here was not smooth. In February 2026, then-CBER director Vinay Prasad issued a rare Refusal-to-File (RTF) letter, citing Moderna's use of a standard-dose comparator in its Phase 3 trial rather than a high-dose comparator. Within days, after public backlash and a formal Type A meeting between Moderna and the FDA, the agency reversed course and accepted the application. Both Prasad and FDA Commissioner Marty Makary have since left the FDA; the June 18 hearing reflected a notably more conventional regulatory posture from the current interim leadership. 5
Panel members were direct about their confidence. Dr. Flor Munoz-Rivas of Baylor College of Medicine said: "I do believe the data presented support that the benefits of the vaccine in both age groups outweigh the risks." 2 Dr. Paul Offit, former VRBPAC member and director of the Vaccine Education Center at Children's Hospital of Philadelphia (CHOP), called it "such a breath of fresh air, considering what we've gone through with Robert F. Kennedy Jr." 1
Moderna's Stéphane Bancel said the company believes "mRNA-1010 has the potential to provide an important new option for seasonal flu prevention." 6
Regulatory filings for MFLUSIVA are also under active review in the EU, Canada, and Australia. 2

What this means for your family: The August 5 date is the one to watch. If the FDA approves MFLUSIVA by then, adults 50 and older will have a genuinely new option for fall — the first flu vaccine built on the mRNA platform that has already delivered over 6 billion COVID-19 doses globally. Mark the date and check back in early August.
The trial data behind the vote
VRBPAC based its recommendation on the FLUENT Phase 3 trial (NCT06602024), a 40,703-person double-blind study conducted across 301 sites in 11 countries. Participants were adults 50 and older; the trial ran across the 2024–2025 flu season, a severe season that accelerated case accrual beyond the target. 8
The headline results:
- Primary efficacy (relative vaccine efficacy, or RVE, vs. standard-dose flu shot): 26.6% (95% confidence interval: 16.7–35.4) against PCR-confirmed flu illness. This met all three pre-specified success criteria: noninferiority, superiority, and a higher-level superiority bar. 8
- Efficacy against severe outcomes (emergency room visits, hospitalizations, urgent care): 47.9% better than the standard-dose comparator. 2
- Median follow-up: 181 days.
One important note on the comparison: MFLUSIVA was tested against standard-dose flu shots, not the high-dose formulation (Fluzone High-Dose) already recommended for adults 65+. Some VRBPAC panelists raised this gap. The confirmatory study required for the 65+ accelerated-approval pathway — enrolling up to 800,000 participants across two flu seasons — is expected to fill that comparison. 4
Side effects: The mRNA vaccine produced more noticeable short-term reactions than the standard-dose comparator: injection-site pain (65.8% vs. 29.8%), fatigue (45.1% vs. 20.3%), headache (37.8% vs. 18.0%), and muscle aches (35.4% vs. 11.6%). Nearly all were mild to moderate and resolved within a day or two. Serious adverse events occurred in 2.2% of mRNA-1010 recipients and 1.9% of comparator recipients; FDA reviewers found no major safety issues or deficiencies. 8
VRBPAC member Dr. Anna Durbin of Johns Hopkins — who voted yes — put the platform clearly: "There were no shortcuts taken. There was a full efficacy evaluation done per standard FDA guidance — phase 3 efficacy studies conducted in tens of thousands of individuals." 1 On the concern about mRNA vaccines that lingers since COVID-19, Dr. Jesse Goodman — former director of FDA's Center for Biologics Evaluation and Research (CBER) — addressed it directly: claims that mRNA vaccines cause cancer or integrate into human DNA "are not possible [and] disproven." 1
A separate advantage the panel found compelling: mRNA manufacturing can compress the strain-to-shot timeline from the current ~6 months down to 2–3 months, closer to the speed achieved with COVID-19 vaccines. That speed advantage could reduce the mismatch risk that hurt standard flu shots in 2024–2025. Several panelists also cited pandemic preparedness as a reason for their yes vote — a faster manufacturing platform means a faster response to a novel strain. 1
A Nature Immunology paper published June 15 — led by Ali Ellebedy and Hanover Matz at Washington University School of Medicine — adds mechanistic depth to these trial results. The study (75 adults, two flu seasons) found that mRNA-1010 induced sustained germinal center reactions — the immune process that generates long-lasting B cells and antibodies — persisting at least 26 weeks in 5 of 13 participants. Recipients of standard Fluarix showed no persistent germinal center response. Antibodies from the mRNA group also recognized a broader range of antigenically different flu strains across decades of viral evolution. 9 Ellebedy described the implication: "If we can make flu immunity broader and more durable, that could mean fewer hospitalizations and deaths." 10
What this means for your family: Adults 50 and older are the target population. The side effects are more pronounced than a standard flu shot — plan for a sore arm, possible fatigue, and maybe a day where you feel run-down. That is the immune system working. The evidence that these temporary reactions buy meaningfully better protection, especially against hospitalization, is solid.
The ACIP complication: FDA approval alone doesn't guarantee coverage
There is a catch that every family planning around MFLUSIVA's August deadline needs to understand.
In the normal approval process, after VRBPAC recommends a vaccine and the FDA approves it, the CDC's Advisory Committee on Immunization Practices (ACIP) — the panel that sets the official US vaccine schedule — votes to recommend the vaccine for specific populations. That ACIP recommendation is what triggers the ACA's preventive services provision, requiring private insurers and Medicare Part D to cover the vaccine at no cost to patients.
ACIP has not held a meeting since December 4–5, 2025 — the longest gap between meetings in decades. 11 A federal district court ruling in March 2026 blocked the Kennedy-reconstituted ACIP from meeting after concluding the 13 members Secretary Kennedy appointed had no vaccine-related expertise. The case — AAP v. Kennedy, First Circuit Case No. 26-1503 — has a joint status report due June 24 (this Tuesday); briefing continues through July 16. 12
An ACIP June 24–26 meeting is listed on CDC's website, but as of June 22, no agenda has been posted, no public comment docket opened, and no presentation materials uploaded — the CDC page has not been updated since February 26. 13 CIDRAP noted last week that "it doesn't appear a meeting will occur." 11
HHS Secretary Kennedy has argued ACIP is "without a quorum" and cannot function. The American Academy of Pediatrics (AAP) calls that a red herring. AAP President Dr. Andrew Racine said: "The federal government has had and continues to have the power to restore a lawful ACIP and schedule a meeting at any time." AAP legal counsel Richard Hughes IV added that Kennedy "wants only the unlawful one and is using a self-created crisis to rush reinstatement of those unlawful appointments." 14
Dr. Durbin, who sat on the VRBPAC panel, put the practical gap plainly: "Right now it's not clear how recommendations would be made for the fall." 1
In the meantime, a newly formed independent body called the SAVRR Council (Summit Adult Vaccine Recommendations Review) held its first public webinar June 9 and voted to advise healthcare professionals to follow current 2025–26 respiratory vaccine recommendations until medical societies — AAP, AAFP, ACOG, and IDSA — publish updated 2026–27 guidance in early September. 15
What this means for your family: FDA approval on August 5 makes MFLUSIVA legal to prescribe. Insurance coverage is a separate question that depends on ACIP — and ACIP's status remains uncertain. If you are 50 or older and want MFLUSIVA this fall, watch for two separate signals: (1) the FDA approval announcement around August 5, and (2) any news about ACIP reconstituting or issuing guidance. Without ACIP acting, you may need to check with your insurer whether the vaccine is covered before scheduling.
Measles: 2,104 cases, still 184 short of the 2025 record
As of June 18, the CDC's case tracker shows 2,104 confirmed measles cases in 2026 — up 31 from 2,073 the prior week, a pace of roughly 4.4 new cases per day. 16 That rate is slower than the ~6 per day recorded earlier in June.
The 2025 full-year record stands at 2,288; the gap is now 184 cases. At the current pace, the 2026 total would cross 2,288 in about 42 days — around early August — though the summer travel season could accelerate spread. 16
The snapshot: 41 jurisdictions reporting cases (one new jurisdiction added this week); 30 active outbreaks; 93% of 2026 cases are outbreak-associated; 92% of cases involved people who were unvaccinated or whose vaccination status was unknown. Zero deaths in 2026 so far. 16
What this means for your family: With school out and summer travel beginning, the measles picture matters. Two doses of MMR (measles-mumps-rubella) vaccine are 97% effective against measles. If any family member is unvaccinated or has only one dose — including children 12 months and older who haven't had their first shot, or anyone born after 1956 who has never been vaccinated — confirm their status before flying anywhere or attending large events. The virus is circulating actively across 41 jurisdictions.
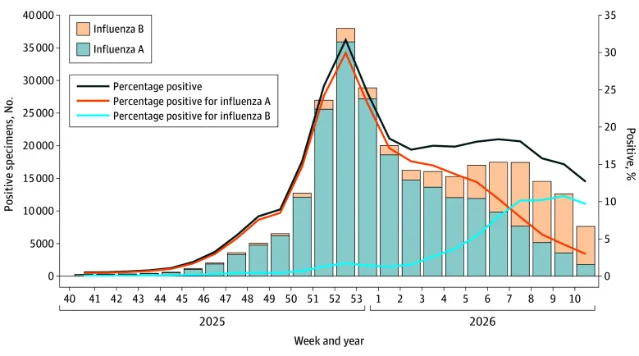
FluView Week 23: summer floor, 182 pediatric deaths
CDC's FluView Week 23 (data through June 13, published June 22) confirms seasonal flu activity is at its off-season minimum. 17
Flu-like illness (ILI) dropped to 1.2% of outpatient visits, down from 1.4% the prior week. All 54 reporting jurisdictions are at minimal activity. Clinical lab positivity: 0.8% (230 of 28,787 specimens tested). Of subtyped influenza A, H3N2 made up 72.0%. 17
Three delayed reports pushed the season's confirmed pediatric flu death count to 182, up from 179 last week — the new deaths occurred in January and February 2026 but were only now reported. 17 The overall 2025–26 season burden: roughly 32 million US flu cases, 390,000 hospitalizations, and 24,000 deaths — with approximately 85% of those eligible for vaccination not fully vaccinated when flu circulated. 1
H5N1 (bird flu): No new human cases this week; the US total remains at 71 confirmed cases since February 2024, including 1 death. CDC's surveillance systems confirmed zero new H5 detections in people for approximately 8 consecutive weeks. 18 Idaho dairy herds reported new H5N1 cattle detections as of June 16; Florida issued an emergency rule requiring negative H5N1 tests for incoming lactating dairy cattle. 19 Person-to-person transmission has not been identified in the US. 17
Vaccine effectiveness for the season just ended: A CDC-led study published June 17 in JAMA Network Open found that H3N2 subclade K (J.2.4.1) dominated in 2025–26, making up 92.7% of genetically characterized H3N2 viruses.
What this means for your family: Flu is not circulating now; this is normal for late June. The season that just ended was severe partly because of the H3N2 mismatch. Both the JAMA study and the FLUENT trial data reinforce that the 2026–27 season — particularly for adults 50+ — would benefit from a more effective vaccine option.
Iowa SF 304: 9 days left for minors to self-consent for HPV and hepatitis B vaccines
Iowa SF 304 takes effect July 1, 2026 — nine days from now. 21 Once the law is in effect, minors in Iowa can no longer consent on their own to vaccines for sexually transmitted infections — specifically the HPV vaccine (which prevents more than 90% of HPV-related cancers, including cervical cancer) and the hepatitis B vaccine. A parent or legal guardian must either be present or provide written consent. 22
The HPV vaccine (Gardasil 9) is recommended starting at ages 11–12, with catch-up dosing through age 26. Most teens who began the series but haven't completed all doses still have time to finish this week, but not much.
As CIDRAP noted, this law creates a patchwork: "A teenager in Iowa who wants to receive the HPV vaccine now needs parental consent to receive it. Meanwhile, a child in Maine can receive it at a pharmacy without a prescription." 22
What this means for your family: Iowa families specifically — if you have a teenager who has started the HPV or hepatitis B series but hasn't finished all doses, call your pediatrician or pharmacy today. After June 30, a parent or guardian must be present or have provided written consent for those appointments.
5 actions to take this week
- Adults 50+: mark August 5 on your calendar. That is the FDA's decision deadline for MFLUSIVA. If approved, ask your doctor or pharmacist in September about availability and, separately, whether your insurance covers it. If ACIP has not acted by then, coverage will vary by insurer. 4
- Iowa families with teenagers: act before June 30. Iowa SF 304 takes effect July 1, removing minors' ability to self-consent for HPV and hepatitis B vaccines. If your teenager needs any remaining doses, schedule before the deadline or make sure a parent can attend. 21
- Check MMR status before summer travel. Measles is at 2,104 cases across 41 jurisdictions. The virus spreads in airports, theme parks, and international destinations where outbreaks are active. Anyone 12 months or older who is unvaccinated or has only one dose should get vaccinated before travel. 16
- Adults 65+ already due for a flu shot this fall: stick with high-dose or adjuvanted. MFLUSIVA may be approved, but it wasn't directly compared to Fluzone High-Dose or Fluad in the Phase 3 trial. Until that confirmatory data exists, the SAVRR Council advises following existing 2025–26 recommendations. High-dose and adjuvanted flu shots remain the recommended choice for adults 65 and older. 15
- Backyard poultry households: mention bird exposure to any doctor visit. H5N1 remains at 71 total US human cases with no new cases in ~8 weeks, but cattle detections continue in Idaho and other states. Standard rapid flu tests miss avian influenza in upper-airway samples. If someone in your household has regular contact with birds and develops respiratory symptoms, tell the doctor explicitly — that context changes the diagnostic approach. 18
Cover image: AI-generated editorial illustration.
参考ソース
- 1NPR: Key FDA committee unanimously recommends its first vaccine since 2023
- 2BioPharm International: FDA Advisory Panel Votes 9-0 in Favor of Moderna's mRNA Flu Vaccine
- 3FDA: VRBPAC June 18, 2026 Meeting Announcement
- 4BioPharma Dive: Moderna flu vaccine wins unanimous support from FDA panel
- 5FierceBiotech: Amenable FDA briefing docs bode well for Moderna's mRNA flu shot ahead of adcomm
- 6Moderna press release via Yahoo Finance
- 7CIDRAP: Moderna's mRNA flu vaccine gets thumbs up from federal vaccine panel
- 8NEJM: Efficacy and Safety of an mRNA Seasonal Influenza Vaccine in Adults
- 9Nature Immunology: mRNA-based influenza vaccine expands B cell response breadth in humans
- 10WashU Medicine: mRNA flu vaccine offers immune protection against wide array of influenza strains
- 11CIDRAP: HHS asks for expedited appeal of court ruling on US vaccine policy
- 12Georgetown Law: Health Care Litigation Tracker
- 13CDC: ACIP Meeting Information
- 14MedPage Today: AAP Disputes Kennedy's Claim That Vaccine Panel Can't Meet
- 15Immunize.org: IZ Express Issue 1879
- 16CDC: Measles Cases and Outbreaks
- 17CDC FluView: Week 23, ending June 13, 2026
- 18CDC: A(H5) Bird Flu Surveillance and Human Monitoring
- 19Agronews: Florida Enacts Emergency Rule to Protect Dairy
- 20JAMA Network Open / CDC: Influenza Activity and Estimated Vaccine Effectiveness During the 2025-2026 Season
- 21Yahoo News / KARE 11: Iowa laws going into effect July 1
- 22CIDRAP/Unbiased Science: The State of US Vaccine Policy — Jun 11, 2026
関連コンテンツ

Five FDA actions in five days: approvals, June 6–11, 2026
FDA Approval: New Drugs & Medical Devices記事
Hantavirus Global Situational Briefing — June 16, 2026
Hantavirus Global Outbreak Monitor記事
The FDA just approved the first new sunscreen ingredient in 25 years. Here's what actually changed.
Gen Z Health Daily記事
このコンテンツについて、さらに観点や背景を補足しましょう。