
2026/6/25 · 9:23
Four NEJM trials and a plasma immunotherapy signal
June 25: NEJM breaks its 7-day drought with four original trials — CAR T at 10 years, RR-TB 6-month regimen, PFA vs antiarrhythmics for persistent AF, and TXA in major noncardiac surgery — plus a Nature Medicine metabolomics study pinpointing plasma histidine as a cross-tumor ICI response predictor.

リサーチノート
Four papers from NEJM's first issue after a 7-day dry spell—covering CAR T-cell durability at a decade, a shorter RR-TB regimen, pulsed-field ablation for persistent AF, and hospital-wide TXA policy—appear alongside a massive metabolomics study from Nature Medicine that identifies plasma histidine as the dominant predictor of immunotherapy outcomes across five solid-tumor types.
At a glance
| # | Paper | Journal | Design | N | Primary finding |
|---|---|---|---|---|---|
| 1 | 10-yr CAR T outcomes (tisagenlecleucel) | NEJM | Single-arm long-term follow-up | 38 | 10-yr lymphoma-free survival: 32% DLBCL, 47% FL |
| 2 | BEAT Tuberculosis (6-month RR-TB) | NEJM | Phase 3 open-label pragmatic RCT | 403 | 86.1% vs 86.0% success; non-inferior (adj. RD −0.2 pp) |
| 3 | AVANT GUARD (PFA for persistent AF) | NEJM | International multi-centre RCT | 310 rand. (+ 50 safety) | 12-month success: 56% PFA vs 30% AAD, HR 0.46 |
| 4 | TRACTION (TXA noncardiac surgery) | NEJM | Cluster-crossover RCT | 8,273 | RBC transfusion 7.4% vs 9.8%, RR 0.73; VTE non-inferior |
| 5 | Plasma histidine & immunotherapy | Nat Med | Multi-cohort metabolomics + ML | 1,714 (4,336 samples) | AUC 0.88 training / 0.73 external validation; CheckMate-025 PFS P=0.007 |
統計カードを読み込んでいます…
Paper 1 — Ten-year outcomes after tisagenlecleucel for B-cell lymphomas
Journal: New England Journal of Medicine 2026;394:2440–2448 | IF tier: Tier 1 (IF ~100) | CME article
Study design: Single-arm, long-term follow-up of the original tisagenlecleucel (CTL019) cohort. 38 patients with relapsed/refractory B-cell NHL — 24 large B-cell lymphoma (LBCL), 14 follicular lymphoma (FL). Data cut-off October 1, 2025; median follow-up 10.1 years (range 7.9–11.5). Lead author: Marco Ruella (University of Pennsylvania). 1
Key findings:
- 10-year lymphoma-free survival: LBCL 32% (95% CI 14–51); FL 47% (95% CI 20–71). 1
- 10-year progression-free survival (including all-cause death): LBCL 17% (95% CI 5–34); FL 29% (95% CI 9–52). 1
- 10-year overall survival: LBCL 17% (95% CI 5–34); FL 50% (95% CI 23–72). 1
- No relapse observed after 5.4 years, establishing a functional cure plateau. 1
- 10-year non-relapse mortality 18% (14% excluding COVID-19-related deaths). Second primary cancers: 9/38 patients, 10-year cumulative incidence 21%. 1
- Persistent grade 2–3 neutropenia in 2 patients (5%); no late-onset anaemia or thrombocytopenia. 44% of durable responders had ongoing B-cell aplasia. 1
Clinical implications: The relapse-free plateau after 5.4 years — unprecedented for a single infusion in multiply relapsed NHL — suggests tisagenlecleucel confers durable remission comparable to allogeneic SCT in FL, without the transplant-related mortality. The 21% second-malignancy rate at 10 years warrants structured surveillance protocols beyond year 5, particularly given the CAR T recipient's chronically immunosuppressed state. Persistent B-cell aplasia in nearly half of long-term responders has practical consequences for infection risk stratification and immunoglobulin replacement planning.
Limitations: 38 patients, single-arm, no contemporaneous comparator. LBCL OS at 10 years (17%) reflects high competing mortality from second primaries and COVID-19 rather than lymphoma progression, and the two subgroups should not be directly compared without accounting for baseline differences.
Paper 2 — BEAT Tuberculosis: 6-month strategy for rifampicin-resistant TB
Journal: New England Journal of Medicine 2026;394:2429–2439 | IF tier: Tier 1 | Funded by USAID
Study design: Phase 3, open-label, pragmatic, randomised, controlled non-inferiority trial conducted in South Africa. 432 screened; 403 randomised (203 experimental, 200 control). Both arms were guided by second-line DST results. Enrolled pregnant/breastfeeding women and fluoroquinolone-resistant TB patients. Non-inferiority margin 10 percentage points. Lead author: Francesca Conradie (University of the Witwatersrand, Johannesburg). 2
Intervention: Bedaquiline + linezolid + delamanid + levofloxacin and/or clofazimine for 6 months vs. South Africa's 9-month standard-of-care regimen.
Key findings:
- Successful outcome (cure or treatment completion at 76 weeks): 174/202 (86.1%) experimental vs 172/200 (86.0%) control; adjusted risk difference −0.2 pp (95% CI −6.9 to 6.5); non-inferiority P=0.001. 2
- Grade ≥3 adverse events: 63/202 (31.2%) experimental vs 74/200 (37.0%) control — numerically fewer in the shorter arm. 2
- Deaths: 10 in each arm. 2

Clinical implications: Cutting RR-TB treatment from 9 to 6 months with an all-oral regimen that included pregnant and FQ-resistant patients — historically excluded from trial populations — directly expands the guideline-eligible population. South Africa already uses bedaquiline-based backbones; this trial provides the non-inferiority evidence needed to shorten duration without worsening outcomes. If adopted, treatment burden drops by three months per patient — consequential for retention in resource-limited settings. Linezolid's peripheral neuropathy and myelosuppression risk require monitoring even in this condensed regimen.
Paper 3 — AVANT GUARD: pulsed-field ablation as first-line therapy for persistent AF
Journal: New England Journal of Medicine 2026;394:2407–2418 (online April 25, 2026) | IF tier: Tier 1 | Funded by Boston Scientific | CME article
Study design: International, multicentre RCT. Drug-naïve persistent AF patients randomised 2:1 to PFA (pentaspline catheter) or antiarrhythmic drugs (AAD); separate PFA-only safety cohort also enrolled. All patients received an implantable cardiac monitor (ICM). Primary efficacy: composite of short-term and long-term treatment success at 12 months. Primary safety: device/procedure-related serious adverse events (combined PFA cohort). Lead author: Oussama Wazni (Cleveland Clinic). 3
Key findings:
- 12-month treatment success: 128/207 PFA (KM 56%, 95% CI 48–63) vs 40/103 AAD (KM 30%, 95% CI 21–40); composite failure HR 0.46 (95% CI 0.33–0.65; P<0.001). 3
- Primary safety (combined PFA cohort, N=257): 13/257 (5.1%) device- or procedure-related serious adverse events. 3
- 12-month serious adverse events overall: PFA 45/207 (25%) vs AAD 20/103 (21%), with no breakdown by type available from the abstract. 3
Clinical implications: Persistent AF has historically been managed with AAD before ablation is offered, in part due to RF ablation's complication profile and operator variability. AVANT GUARD's near-halving of composite failure risk (HR 0.46) with PFA as the initial strategy challenges that stepwise paradigm. PFA's mechanism — irreversible electroporation rather than thermal injury — is associated with reduced collateral damage to the oesophagus and phrenic nerve, which may explain both the efficacy and the modest safety event rate. The ICM-verified endpoint (rather than symptom-reported outcomes) strengthens the signal. The 5.1% device/procedure SAE rate in the ablation arm is the number operators will scrutinise most carefully against their centre's RF complication benchmarks.
Paper 4 — TRACTION: hospital-wide TXA policy cuts transfusion in noncardiac surgery
Journal: New England Journal of Medicine 2026;394:2419–2428 (online June 10, 2026) | IF tier: Tier 1 | Funded by CIHR + Ontario MOHLTC
Study design: Multi-centre, double-blind, cluster-crossover RCT (hospital as the randomisation unit, switching every 4 weeks). 10 Canadian hospitals, 8,273 patients undergoing major noncardiac surgery at high risk for RBC transfusion. Oncological surgery: 60.5% of participants. Co-primary endpoints: (1) in-hospital RBC transfusion (superiority), (2) 90-day VTE diagnosis (non-inferiority; margin RR 95% CI upper limit 1.46). Lead author: Breanna Houston (University of Manitoba). 4
Key findings:
- RBC transfusion: TXA 7.4% (306/4,156) vs placebo 9.8% (403/4,117); RR 0.73 (95% CI 0.61–0.86); adjusted difference −2.7 pp (95% CI −4.2 to −1.4). 4
- 90-day VTE: TXA 2.1% (86/4,128) vs placebo 2.1% (85/4,052); RR 0.96 (95% CI 0.65–1.38); adjusted difference −0.1 pp — non-inferiority criterion met. 4
Clinical implications: TXA has an established evidence base in cardiac and orthopaedic surgery; TRACTION extends that evidence to a broad, unselected noncardiac surgical population at the hospital-policy level rather than on a case-by-case basis. The cluster-crossover design captures real-world implementation effects across surgical specialties simultaneously. The absolute risk reduction of 2.7 pp translates to roughly 1 avoided transfusion per 37 patients treated — meaningful at scale given the ~30 million major noncardiac operations performed in North America annually. Critically, the VTE non-inferiority result addresses the longstanding concern that antifibrinolytic agents promote clotting complications in oncology patients (60.5% of the cohort). Hospitals without a TXA policy for noncardiac surgery now face a clear evidence gap to justify its absence.
Paper 5 — Plasma histidine predicts immunotherapy outcomes across solid tumors
Journal: Nature Medicine 2026 (online June 25) | IF tier: Tier 1 (IF ~82) | Open access | Corresponding author: Laurence Zitvogel (Gustave Roussy, Villejuif, France) 5
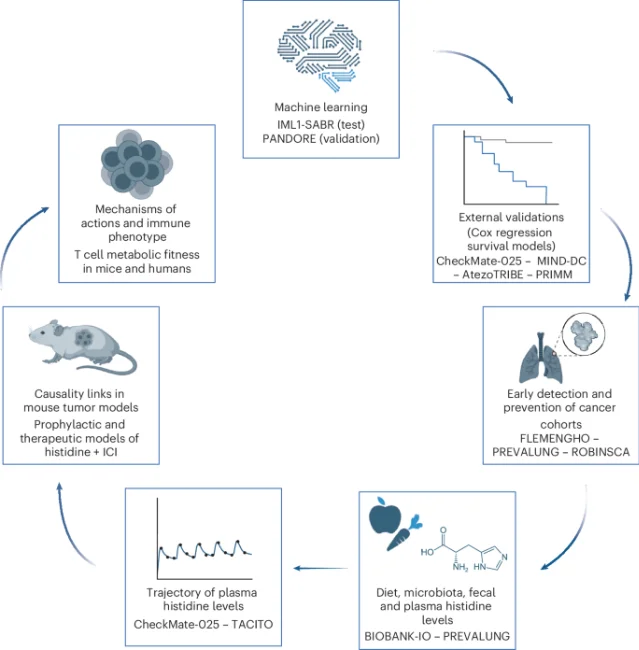
Study design: Multi-cohort, mass spectrometry-based targeted metabolomics study — the largest immunotherapy metabolomics dataset assembled to date. 1,714 patients, 4,336 plasma samples across 5 tumor types (lung, colon, kidney, bladder, skin) and 16 cohorts (Europe + North America), covering five ICI-based treatment modalities including FMT. A supervised ML model (DynForest) integrated 154 metabolites and clinical variables. Lead author: Déborah Suissa (Gustave Roussy). 5
Key findings:
- 8-predictor signature (DynForest model): histidine, succinic acid, carnitine, docosatrienoic acid, hexadecanedioic acid, creatinine, age, BMI. Training AUC 0.88 (IML1+SABR, n=105); external validation AUC 0.73 (PANDORE, n=30); generalised across 7 external cohorts. 5
- Histidine = dominant favourable prognostic feature; long-chain fatty acids and succinate were unfavourable. 5
- Histidine supplementation enhanced antitumour immunity in mice; histidine-rich diets improved PFS in patients without dysbiotic microbiome. 5
- CheckMate-025 validation (nivolumab vs. everolimus in renal cell carcinoma, n=743): higher baseline histidine strongly associated with better PFS and OS; significant treatment-arm interaction P=0.007 for PFS, P=0.002 for OS. 5
- Authors attribute histidine's role to protein-rich diets and microbiota fitness, linking gut ecology to systemic metabolic readiness for ICI response. 5
Clinical implications: A reliable pre-treatment plasma biomarker generalising across five solid-tumor types and five ICI modalities fills a persistent gap in oncology: current PD-L1 and TMB assays perform poorly outside their index tumor type. A plasma histidine measurement is simpler and cheaper than tissue-based assays. The treatment-arm interaction in CheckMate-025 suggests histidine does not merely mark overall fitness — it appears to specifically enrich response to nivolumab over everolimus, making it potentially actionable for treatment selection in RCC. The dietary and microbiome mechanism opens a trial-amenable intervention arm (histidine supplementation), though efficacy in patients with baseline dysbiosis still needs prospective investigation.
Limitations: Training cohort size (n=105) is small relative to the 8-predictor model complexity; external validation AUC (0.73) is lower than training (0.88), consistent with overfitting not yet fully resolved. Causal direction between histidine levels and ICI response — microbiome fitness as confounder vs. direct immunomodulatory mechanism — is not established in the human data.
Cover image: Laboratory centrifuge specimen processing via Pexels.
参考ソース
- 1Ten-Year Outcomes after CAR T-Cell Therapy for B-Cell Lymphomas — PubMed
- 2A Pragmatic Trial of a 6-Month Strategy for Rifampicin-Resistant Tuberculosis — PubMed
- 3Pulsed Field Ablation as Initial Therapy for Persistent Atrial Fibrillation — PubMed
- 4Hospital Policy of Tranexamic Acid to Reduce Transfusion in Major Noncardiac Surgery — PubMed
- 5Metabolic determinants of cancer immunotherapy outcomes identified by plasma profiling — Nature Medicine


このコンテンツについて、さらに観点や背景を補足しましょう。