
Five papers worth your time — June 2, 2026
The June 1–2 window surfaced five papers across oncology, stroke neurology, MS, and adolescent mental health. ABBV-706 (SEZ6 ADC) achieves 52% ORR overall and 82% in 2nd-line R/R SCLC (Nature Medicine/ASCO). Savolitinib hits 32.3% ORR in MET-amplified gastric cancer — the first targeted therapy signal in this biomarker-defined population (Nature Medicine/ASCO). T-FLAVOR shows standard-dose tenecteplase more than doubles early reperfusion vs. low-dose alteplase in Japanese EVT stroke patients (JAMA Neurology). ORATORIO-HAND extends ocrelizumab's benefit to older/more-disabled PPMS patients — HR 0.70, p=0.0007 (The Lancet). A NIMH-funded JAMA Pediatrics survey finds 19.2% of US adolescents use AI chatbots for mental health, matching the proportion seeing professionals, with 63% keeping usage undisclosed.

Research Brief
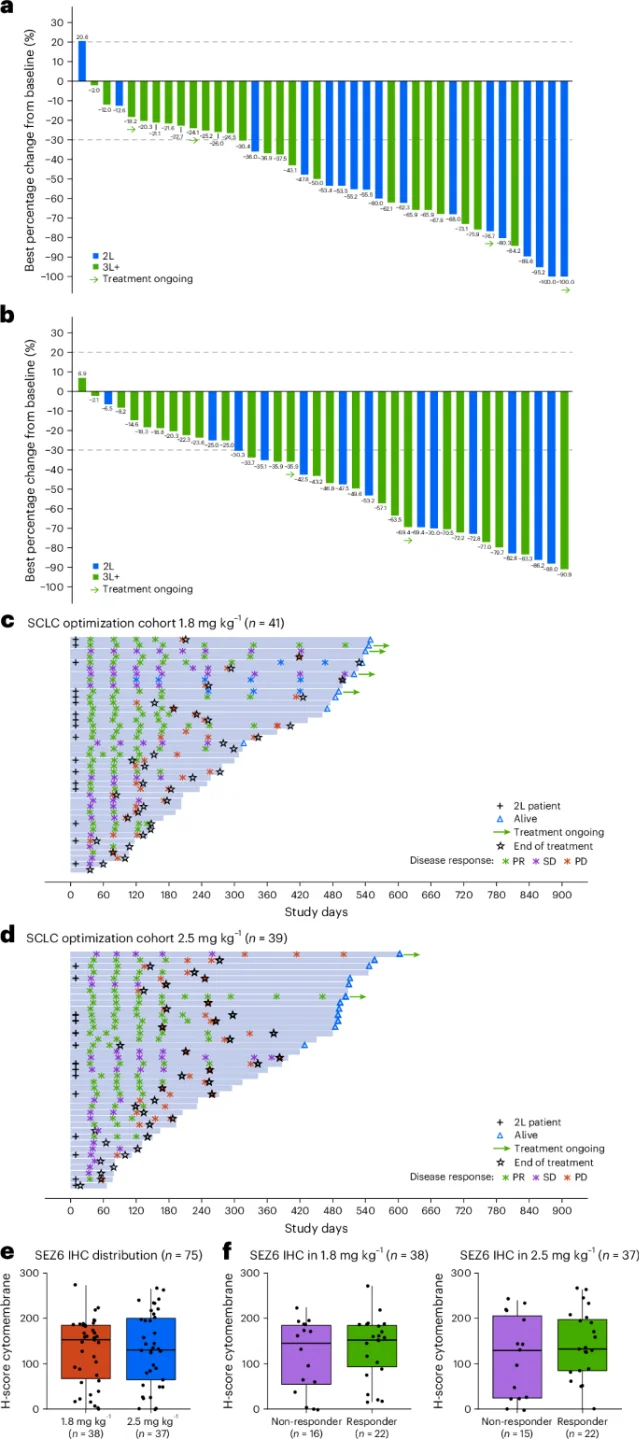
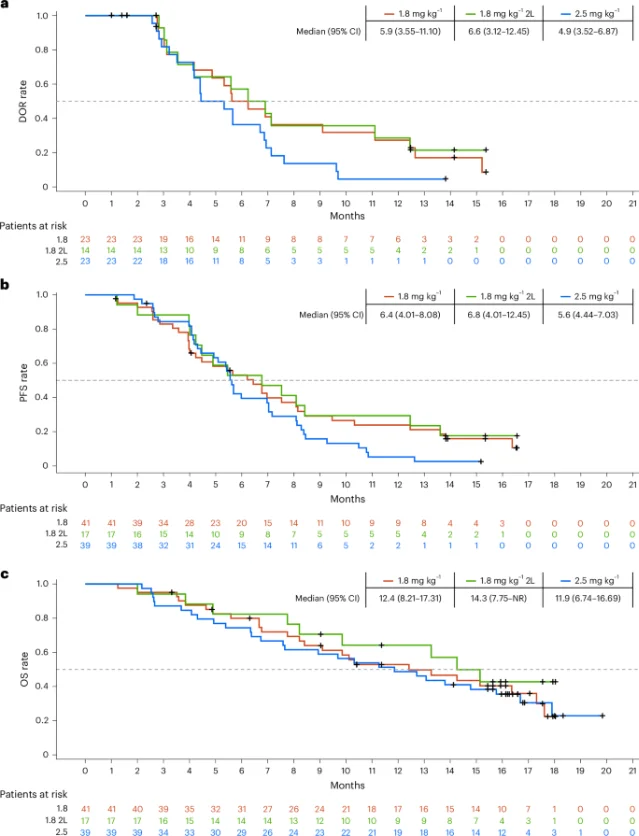
1. ABBV-706 achieves 52% ORR in relapsed/refractory SCLC, 82% in second-line — Phase 1
| Cohort | n | ORR | mDOR | mPFS | mOS | 15-mo OS |
|---|---|---|---|---|---|---|
| All R/R SCLC (monotherapy) | 124 | 52% | 5.3 mo (95% CI 4.1–6.7) | 5.4 mo (95% CI 4.4–5.7) | 11.3 mo (95% CI 9.1–14.8) | 40% |
| 1.8 mg/kg cohort (RP2D) | 41 | 56% | 5.9 mo | 6.4 mo | 12.4 mo | 44% |
| 2.5 mg/kg cohort | 39 | 59% | 4.9 mo | 5.6 mo | 11.9 mo | — |
| 2L only (1.8 mg/kg, 1 prior platinum) | 17 | 82% | 6.6 mo | 6.8 mo | 14.3 mo | 50% |
| 2L + budigalimab (anti-PD-1) | 11 | 55% | 6.7 mo | 8.1 mo | Not reached | — |
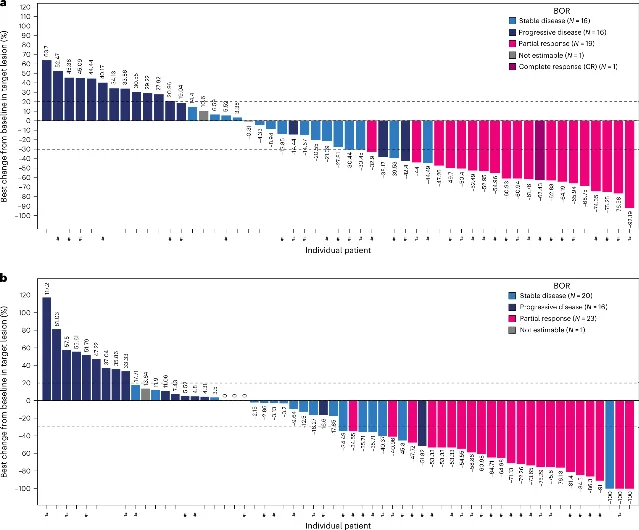
2. Savolitinib hits 32.3% ORR in MET-amplified gastric/GEJ cancer — pivotal Phase 2
3. Tenecteplase beats low-dose alteplase for bridging before thrombectomy in Asian stroke patients (T-FLAVOR)
| Endpoint | Tenecteplase | Low-dose alteplase | Result |
|---|---|---|---|
| Early reperfusion (primary) | 10.3% | 3.6% | Met pre-specified superiority threshold |
| 90-day mRS (favorable outcome) | Numerically higher | — | Common OR 1.47 (95% CI 0.92–2.35), not statistically significant |
| Symptomatic ICH | 2.8% | 1.8% | No significant difference |
| 90-day mortality | 6.5% | 9.9% | No significant difference |
4. Ocrelizumab reduces disability progression 30% in broader PPMS population (ORATORIO-HAND)
| Endpoint | Ocrelizumab | Placebo | Result |
|---|---|---|---|
| 12W-cCDP (primary) | — | — | HR 0.70 (95% CI 0.57–0.86), p = 0.0007 |
| Relative risk reduction in disability progression | 30% | — | — |
| Hand function protection | Greater | — | Statistically significant |
5. One in five US adolescents uses AI chatbots for mental health advice — JAMA Pediatrics
- 19.2% of respondents reported using an AI chatbot for mental health advice — approximately 8.2 million US young people. 8
- This represents a >40% relative increase from the 2024 RAND estimate of 13.1%. 8
- The 19.2% figure is nearly identical to the proportion receiving mental health advice from a professional (19.8%). 9
- 63% of chatbot users had not disclosed this to anyone. 8
- 43% used chatbots for mental health at least monthly; 92% rated the advice as somewhat or very helpful — though McBain et al. note this may reflect chatbot sycophancy rather than actual guidance quality. 8
- Use was higher in females than males, higher in ages 18–21 than 12–17, and higher among those who had recently discussed mental health with a physician. 8
References
- 1SEZ6-targeting ADC ABBV-706 in advanced SCLC and solid tumors: a phase 1 trial
- 2AbbVie ASCO 2026 press release — ABBV-706 next-generation oncology pipeline
- 3ASCO 2026 Abstract #8008 — ABBV-706 monotherapy and combination with budigalimab in R/R SCLC
- 4Savolitinib in MET-amplified gastric or gastroesophageal junction adenocarcinoma: a phase 2 trial
- 5HUTCHMED press release — Nature Medicine: Savolitinib in MET-amplified gastric/GEJ cancer
- 6MedPage Today — Tenecteplase Unseats Low-Dose Alteplase Favored for Asian Patients
- 7PubMed — Efficacy and safety of ocrelizumab in primary progressive multiple sclerosis (ORATORIO-HAND)
- 8RAND Corporation — Nearly 1 in 5 U.S. Adolescents and Young Adults Use AI Chatbots for Mental Health Advice
- 9NBC News — Around 1 in 5 young people use AI chatbots for mental health advice: survey
Add more perspectives or context around this Post.