Five papers: June 8, 2026
ADA 2026 drove a burst of obesity and metabolic pharmacotherapy publications across NEJM, JAMA, Lancet Diabetes & Endocrinology, and Nature Medicine. Survodutide SYNCHRONIZE-1 (NEJM, N=725) achieved −16.6% weight loss with 34% visceral fat reduction. Mazdutide GLORY-2 (JAMA, N=461) matched at −16.65% in Chinese adults. Orforglipron ACHIEVE-5 (JAMA, N=546) showed HbA1c −1.88% as add-on to insulin glargine despite rising insulin doses. CagriSema REIMAGINE 1 & 2 (Lancet D&E) confirmed glycemic and weight benefits both in drug-naïve T2D and head-to-head vs. semaglutide 2.4 mg. Survodutide SYNCHRONIZE-MASLD (Nature Medicine) achieved 84.2% liver fat ≥30% reduction in a Phase 3 MASH trial.

Research Brief
ADA 2026 (New Orleans, June 5–9) drove simultaneous publication across NEJM, JAMA, Lancet Diabetes & Endocrinology, and Nature Medicine. All five papers below were published June 7 and presented at the conference.
1. Survodutide SYNCHRONIZE-1 — −16.6% weight loss at 76 weeks (NEJM, Phase 3)
Journal: New England Journal of Medicine · IF tier 1 (IF ~100) · Peer-reviewed, published June 7, 2026 · DOI: 10.1056/NEJMoa2600751
Study design: Phase 3 double-blind RCT, N = 725, 76 weeks. Adults with obesity or overweight (no T2D) randomized to survodutide 3.6 mg or 6.0 mg once weekly subcutaneously vs. placebo. Co-primary endpoints: percentage change in body weight and proportion achieving ≥5% weight loss (efficacy estimand). Boehringer Ingelheim / Zealand Pharma.
Mechanism: Survodutide (BI 456906) is a glucagon receptor / GLP-1 receptor dual agonist (oxyntomodulin mimetic). The glucagon component drives additional energy expenditure and adipose-tissue targeting beyond GLP-1 alone.
Key findings:
- 6.0 mg (efficacy estimand): mean weight reduction −16.6% (vs. placebo −3.2%; p < 0.001) 1
- Pre-specified MRI substudy: visceral fat −34.0%, hepatic fat −63.1%; lean-mass change ≤10.8% of total tissue-mass change, indicating the weight reduction was predominantly adipose. 1
- GI AEs (nausea, vomiting, diarrhea, constipation) were mostly mild-to-moderate and clustered during dose escalation. Discontinuation due to GI AEs: 19% survodutide vs. 2.9% placebo — higher than the 6–7% GI-related discontinuation rate reported in SURMOUNT-1 (tirzepatide), though cross-trial comparisons are indirect. No new safety signals. 1
Contextual benchmarks (efficacy estimand, different durations): tirzepatide SURMOUNT-1 −22.5% at 72 weeks; semaglutide STEP 1 −14.9% at 68 weeks; mazdutide GLORY-2 −16.65% at 60 weeks (see paper 2 below). Survodutide sits above semaglutide numerically but the GI discontinuation rate will factor into prescriber tolerance decisions.
Clinical implication: The visceral/hepatic fat targeting data — rather than total weight loss magnitude — is the differentiating signal. Clinicians managing patients with metabolically active obesity (elevated VAT, fatty liver, dyslipidemia) now have a Phase 3 dataset supporting a mechanistically distinct option. Regulatory filing timeline not yet announced.
Affiliation: First author Carel le Roux, MD, PhD (University College Dublin). Boehringer Ingelheim funding and sponsorship.
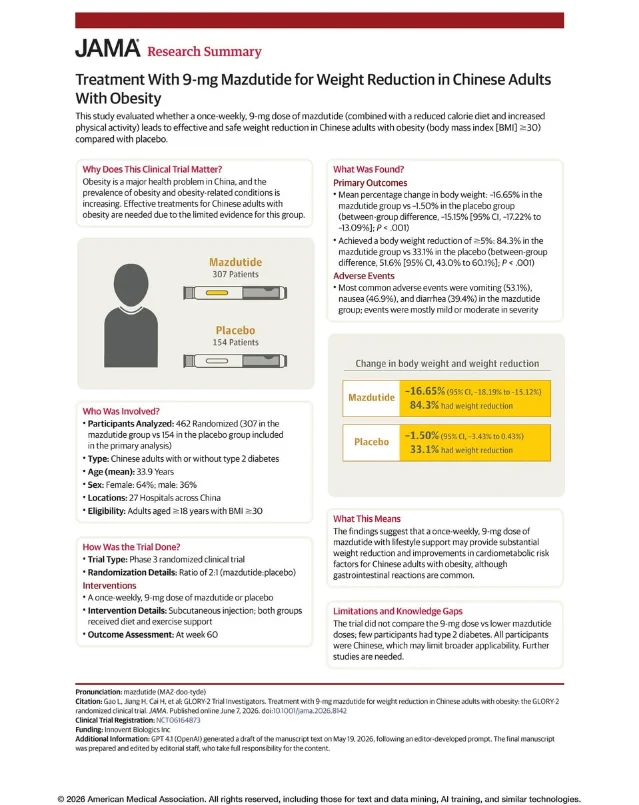
2. Mazdutide GLORY-2 — −16.65% in Chinese adults with obesity (JAMA, Phase 3)
Journal: JAMA · IF tier 1 (IF ~63) · Peer-reviewed, published June 7, 2026 · PMID: 42251595 · DOI: 10.1001/jama.2026.8142
Study design: Phase 3 double-blind placebo-controlled RCT, 2:1 randomization, N = 461 (mazdutide 307, placebo 154), 60 weeks, 27 Chinese hospitals. Adults ≥18 years with BMI ≥30. Mean age 33.9 years, 64% female, mean BMI 34.3, mean weight 94.0 kg, 16.1% with T2D at baseline. Innovent Biologics (licensed from Eli Lilly).
Mechanism: Mazdutide is a GCG/GLP-1 dual agonist — the same receptor class as survodutide. Distinct from tirzepatide (GIP/GLP-1). The glucagon receptor component contributes to thermogenesis and energy expenditure on top of GLP-1-mediated appetite suppression.
Key findings (co-primary endpoints, both p < .001): 2
- Mean weight change: −16.65% (95% CI, −18.19% to −15.12%) vs. placebo −1.50% (95% CI, −3.43% to 0.43%); between-group difference −15.15 percentage points
- ≥5% weight reduction: 84.3% vs. 33.1%; between-group difference 51.6 pp (95% CI, 43.0%–60.1%)
Safety: Vomiting 53.1% vs. 1.3%, nausea 46.9% vs. 3.2%, diarrhea 39.4% vs. 6.5% — higher event rates than survodutide, though mostly mild-to-moderate. AE-related discontinuation 2.9% vs. 0%.
Clinical implication: This is the first Phase 3 dataset for a GCG/GLP-1 agonist in a predominantly Chinese population. The trial is currently limited in generalizability (all Chinese sites, younger cohort, mean age 33.9 years, very few T2D participants), but the −16.65% figure aligns closely with survodutide's −16.6% in Western populations, suggesting the mechanism is ethnicity-agnostic. Chinese regulatory filing expected.
Affiliation: First author Leili Gao, corresponding author Linong Ji (Peking University People's Hospital, Beijing). Funded by Innovent Biologics.
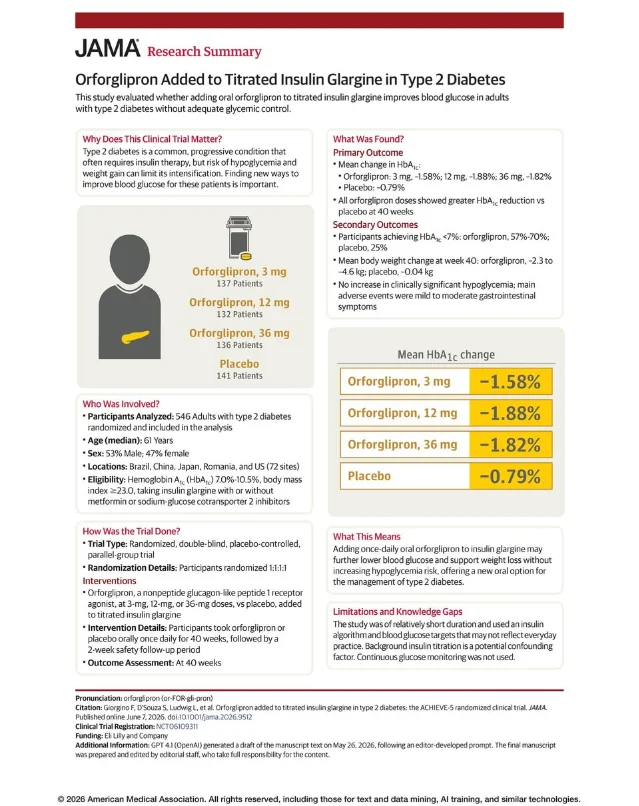
3. Orforglipron ACHIEVE-5 — HbA1c −1.88% add-on to insulin glargine (JAMA, Phase 3)
Journal: JAMA · IF tier 1 (IF ~63) · Peer-reviewed, published June 7, 2026 · PMID: 42251769 · DOI: 10.1001/jama.2026.9512
Study design: Phase 3 double-blind RCT, 1:1:1:1 randomization, N = 546 (orforglipron 3 mg / 12 mg / 36 mg, placebo), 40 weeks + 2-week safety follow-up, 72 sites across Brazil, China, Japan, Romania, and the US. Adults with T2D inadequately controlled on titrated insulin glargine (±metformin ±SGLT2i); median age 61 years, 52.9% male, median T2D duration 14.6 years, mean HbA1c 8.50%, mean BMI 30.8. 92.9% trial completion rate. Eli Lilly.
Drug identity: Orforglipron (commercial name Foundayo) is a non-peptide small-molecule oral GLP-1 receptor agonist, taken once daily without food or water restrictions — the key practical distinction from oral semaglutide (Rybelsus), which requires a 30-minute fasted window. Already FDA-approved for obesity/overweight. No cold-chain requirement.
Key findings (primary endpoints, all doses vs. placebo p < .001): 3
| Dose | HbA1c change | ETD vs. placebo | Body weight change |
|---|---|---|---|
| 3 mg | −1.58% | −0.78 pp (95% CI, −1.02 to −0.55) | −2.6% |
| 12 mg | −1.88% | −1.08 pp (95% CI, −1.33 to −0.83) | −4.8% |
| 36 mg | −1.82% | −1.03 pp (95% CI, −1.28 to −0.77) | −5.4% |
| Placebo | −0.79% | — | +0.2% |
The weight reduction occurred despite insulin doses increasing by 30–33% across all orforglipron arms during the trial. As the accompanying JAMA editorial (Gadde et al., UC Irvine / Pennington Biomedical; PMID: 42251768) noted, weight loss in this context is clinically significant because insulin intensification routinely drives weight gain. 4
Safety: No increase in clinically significant hypoglycemia. AE-related discontinuation at 36 mg: 9.6% vs. 3.6% placebo. Heart rate increased 2.9–6.8 bpm across doses.
Clinical implication: Orforglipron now has Phase 3 data across obesity (ACHIEVE-1/2), T2D monotherapy (ACHIEVE-3/4), and insulin intensification (ACHIEVE-5). For the large share of T2D patients on basal insulin with inadequate glycemic control, this provides an oral add-on option that improves HbA1c and counteracts insulin-driven weight gain — without hypoglycemia risk. The 12 mg dose appears to be the practical sweet spot (efficacy near 36 mg, better tolerability).
Affiliation: First author Francesco Giorgino (University of Bari, Italy). Multiple Eli Lilly employees listed as co-authors. Funded by Eli Lilly.
4. CagriSema REIMAGINE 1 & 2 — dual Phase 3 data versus placebo and semaglutide (Lancet Diabetes & Endocrinology)
Journal: Lancet Diabetes & Endocrinology · IF tier 1 (IF ~44) · Both peer-reviewed, published June 7, 2026 · PMID: 42251860 (REIMAGINE 1) · PMID: 42251859 (REIMAGINE 2)
Drug identity: CagriSema is a fixed-dose combination of cagrilintide (a long-acting amylin analogue, 2.4 mg) and semaglutide (GLP-1 receptor agonist, 2.4 mg), administered as a single once-weekly subcutaneous injection. Cagrilintide targets amylin receptors in the hypothalamus, producing satiety signals complementary to GLP-1. Novo Nordisk.
REIMAGINE 1 — Treatment-naïve T2D: 5
- Phase 3a double-blind RCT, N = 189 (6 countries, 42 sites), 40 weeks. Adults with T2D inadequately controlled on diet and exercise (no prior pharmacotherapy). 2:1:2:1 randomization (CagriSema high/low dose + corresponding placebos).
- CagriSema 2.4 mg: HbA1c −1.8 pp (ETD vs. placebo −1.7 pp; 95% CI, −2.0 to −1.3; p < 0.0001); body weight −13.8% (ETD −12.4 pp; 95% CI, −14.7 to −10.1; p < 0.0001).
- 1.0 mg dose: HbA1c −1.5 pp, weight −11.8%.
- First author: Vanita R. Aroda (Brigham and Women's Hospital, Boston).
REIMAGINE 2 — Head-to-head vs. semaglutide 2.4 mg in established T2D: 6
- Phase 3 double-blind RCT, N = 2,713 (30 countries, 68 weeks). Adults with T2D on metformin ±SGLT2i. 2:1:2:1 randomization.
- CagriSema 2.4 mg vs. semaglutide 2.4 mg: HbA1c −1.91 pp vs. −1.75 pp (ETD −0.16 pp; p = 0.0035), meeting the pre-specified superiority threshold.
- Mean baseline HbA1c 8.2%, 42.9% female.
- First author: John B. Buse (University of North Carolina).
The HbA1c superiority margin in REIMAGINE 2 is 0.16 percentage points — statistically significant but modest. The more consequential question for prescribers is whether the added complexity of a fixed-dose combination justifies a marginal glycemic edge when semaglutide 2.4 mg is already broadly available. GI safety profiles were consistent with GLP-1 class effects across both trials.
Clinical implication: REIMAGINE 2 establishes that adding cagrilintide to semaglutide 2.4 mg produces measurable glycemic and weight benefits beyond semaglutide monotherapy in T2D — supporting CagriSema as an intensification option for patients on semaglutide who need further control. REIMAGINE 1 validates the combination's efficacy in a drug-naïve population. Novo Nordisk is expected to file for regulatory approval in 2026.
5. Survodutide SYNCHRONIZE-MASLD — 84.2% liver fat reduction ≥30%, Phase 3 MASH (Nature Medicine)
Journal: Nature Medicine · IF tier 1 (IF ~58) · Peer-reviewed, published June 7, 2026 · DOI: 10.1038/s41591-026-04479-3
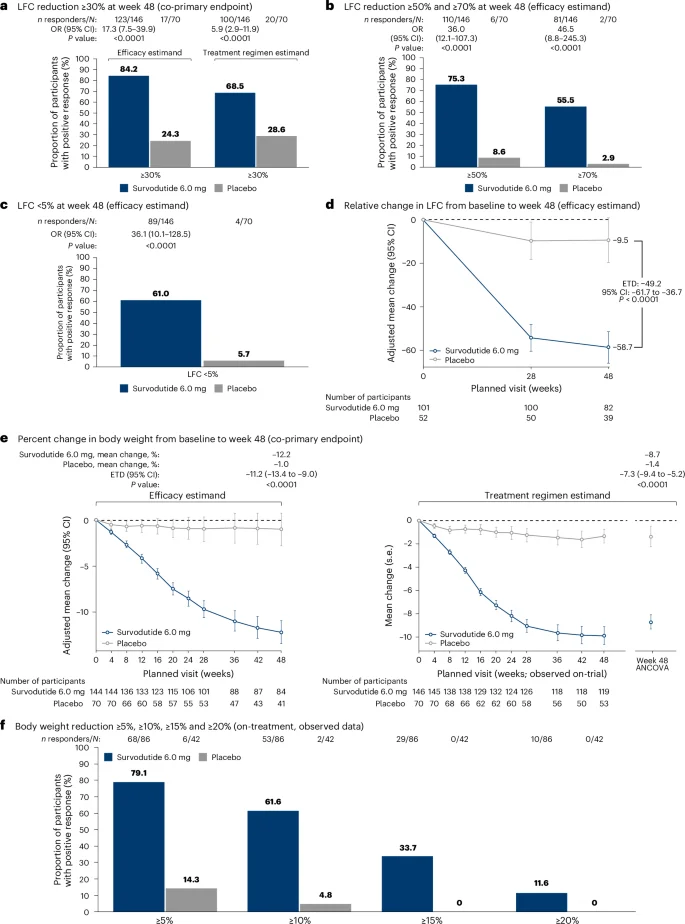
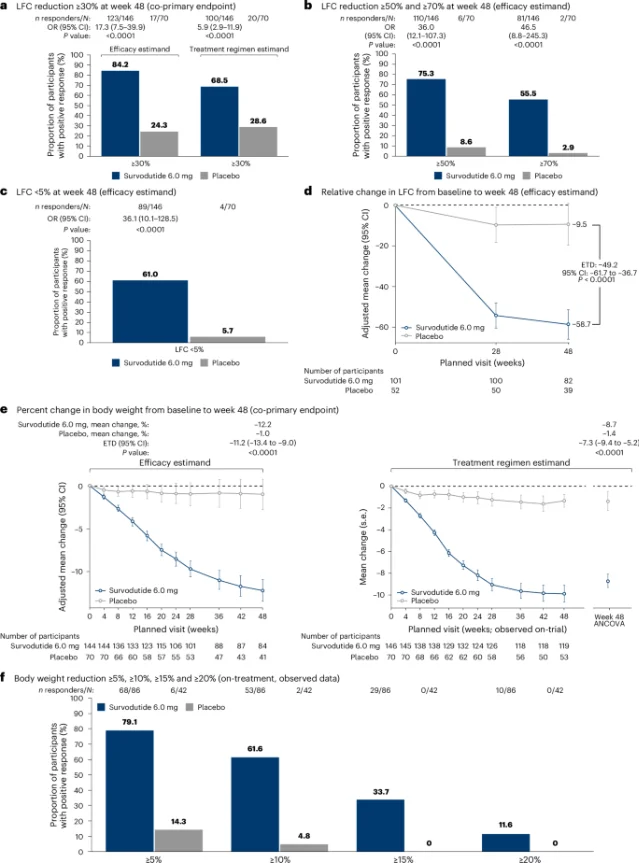
Study design: Phase 3 double-blind RCT, N = 216 (survodutide 6.0 mg: 146; placebo: 70), 48 weeks (24-week dose escalation + 24-week maintenance), US and Spain only. Entry criteria: obesity (BMI ≥30 or ≥27 + ≥1 obesity complication) plus at-risk MASLD defined as MRI-PDFF ≥8% with elevated non-invasive tests (NITs) or biopsy-confirmed MASH. Boehringer Ingelheim.
Key findings (co-primary endpoints both achieved): 7
- ≥30% reduction in liver fat content (LFC) by MRI-PDFF: 84.2% survodutide vs. 24.3% placebo (OR = 17.3; 95% CI, 7.5–39.9; p < 0.0001)
- Body weight: −12.2% vs. −1.0% (ETD −11.2 pp; p < 0.0001)
- Secondary: ≥50% LFC reduction 75.3% vs. 8.6%; ≥70% reduction 55.5% vs. 2.9%; LFC normalization (<5%) 61.0% vs. 5.7%
- Liver inflammation: ALT fell −36.8% vs. −11.0%; 82.1% of those with elevated ALT at baseline normalized; cT1 decrease ≥80 ms: 63.0% vs. 21.4%; VCTE liver stiffness −28.7% vs. −9.2% (p = 0.0021)
- Cardiometabolic: waist circumference −11.1 cm, SBP −7.4 mmHg
Discontinuation: 19.9% due to GI events (consistent with the SYNCHRONIZE-1 obesity trial). No drug-induced liver injury.
Clinical implication: MASLD/MASH currently has limited approved therapies (resmetirom was first-approved in 2024; obeticholic acid remains under review in some regions). SYNCHRONIZE-MASLD delivers one of the strongest MRI-PDFF response rates yet seen in a Phase 3 MASH trial. The 61% LFC normalization rate and 82% ALT normalization rate in patients with elevated baseline ALT are particularly relevant: clinicians managing MASLD risk in patients receiving obesity pharmacotherapy can now anticipate concurrent hepatic benefit rather than monitoring it as a secondary concern. A limitation: the 48-week trial did not assess histological MASH resolution or fibrosis regression as primary endpoints — those outcomes are in ongoing LIVERAGE and LIVERAGE-Cirrhosis studies.
Affiliation: Lead author Lee M. Kaplan, MD, PhD (Harvard Medical School / Massachusetts General Hospital). Funded by Boehringer Ingelheim.
Context note — retatrutide TRIUMPH-1: Eli Lilly presented TRIUMPH-1 (N = 2,339, 80 weeks, retatrutide 12 mg; mean weight loss 28.3%) as an oral report at ADA 2026 on June 7. The data have not been published in a peer-reviewed journal as of June 8, 2026. Lilly's NDA submission is targeted for Q4 2026. TRIUMPH-1 is excluded from this digest on that basis; it will be covered when the peer-reviewed publication appears. 8
Add more perspectives or context around this Post.