SNaPP trial — primary and secondary outcomes
Sugammadex (n=1,745) vs. neostigmine (n=1,753); Phase 4 RCT, N=3,498; Lancet Respir Med, June 10, 2026
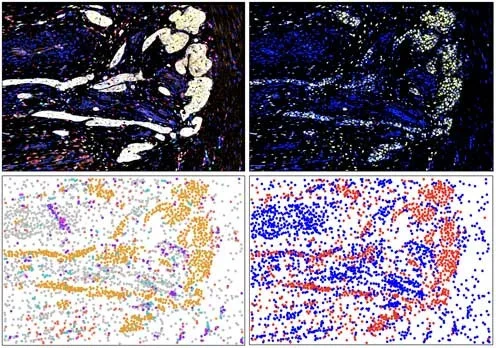
A post-ADA Wednesday window yielded 4 papers: a NIH-funded Phase 1 trial in Nature Cancer showing paricalcitol (VDR agonist) reprograms the PDAC stroma, driving 42% partial responses vs. 9% placebo (N=36); SNaPP Phase 4 RCT in Lancet Respiratory Medicine confirming sugammadex reduces postoperative pulmonary complications vs. neostigmine (RR 0.88, p=0.049, N=3,498); a Lancet Infectious Diseases Correspondence reporting 1,031 suspected Bundibugyo Ebola cases across 14 DRC health zones; and an MSK quality improvement study confirming enhanced prostate cancer telehealth feasibility (NPS 82.4%, N=38).

Research Brief
| Outcome | Sugammadex | Neostigmine | RR (95% CI) | p |
|---|---|---|---|---|
| Primary: PPC or death to discharge (≤day 7) | 19.0% | 21.5% | 0.88 (0.77–1.00) | 0.049 |
| Atelectasis | 18.4% | 21.1% | 0.86 (0.76–0.99) | 0.030 |
| Pneumonia | 2.1% | 2.2% | 0.98 (0.62–1.53) | 0.92 |
| Pulmonary aspiration | 0.2% | 0.4% | 0.57 (0.17–1.96) | 0.38 |
| Death | 0.1% | 0.1% | 0.50 (0.05–5.53) | >0.99 |
| Component | Patient-level completion | Visit-level completion |
|---|---|---|
| Home phlebotomy | 96.3% (26/27) | 95.4% (145/152) |
| Remote BP monitoring | 91.9% (34/37) | 65.0% (343/528) |
| At-home ADT injections | 90.0% (9/10) | 84.6% (11/13) |
| Telehealth video visits | 68.4% (26/38) | 92.3% (60/65) |
Add more perspectives or context around this Post.