Five papers worth your time — June 3, 2026
The June 2–3 window surfaces five papers across rheumatology, thoracic oncology, breast cancer, infectious disease, and pharmacoepidemiology. Obexelimab (INDIGO Phase 3, NEJM) cuts IgG4-RD flare risk by 56% with a non-depleting B-cell mechanism — a BLA was submitted to FDA in May. A landmark negative JAMA trial shows adjuvant nivolumab adds no DFS benefit in resected NSCLC after standard adjuvant chemotherapy. Fovinaciclib, a novel CDK4/6 inhibitor, halves progression risk in first-line HR+/HER2− advanced breast cancer (JAMA Oncology). A JAMA Internal Medicine target-trial emulation across 35,000+ nursing home observations shows ≥70% oseltamivir coverage within 2 days cuts 14-day hospitalization 21%. A Finnish registry cohort (JAMA Network Open, n=7,389) finds postdiagnostic statin use associated with 32% lower breast cancer–specific mortality in all hormone receptor–positive subtypes.

Research Brief
1. Obexelimab cuts IgG4-RD flares by 56% in Phase 3 — NEJM
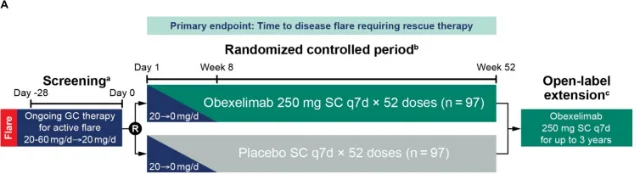
| Endpoint | Obexelimab | Placebo | Result |
|---|---|---|---|
| Time to first adjudicated flare (primary) | — | — | HR 0.44 (95% CI 0.277–0.711); p = 0.0005 |
| 52-week flare-free rate | 73.2% | 45.4% | — |
| Investigator-defined flare (key secondary) | — | — | HR 0.41 (95% CI 0.26–0.66); p = 0.0001 |
| Complete remission at Week 52 | 37.1% | 19.6% | p = 0.0049 |
| Cumulative rescue GC dose | 329.5 mg | 929.8 mg | p = 0.0042 (65% reduction) |
| Grade ≥3 TEAEs | 11.3% | 23.7% | — |
2. Adjuvant nivolumab shows no DFS benefit in resected NSCLC — JAMA
| Endpoint | Nivolumab | Observation | Result |
|---|---|---|---|
| Median DFS, ITT (co-primary) | 71.3 months | 68.8 months | HR 0.97 (97% CI 0.79–1.20); P = 0.39 |
| Median DFS, PD-L1 ≥50% (co-primary) | 89.8 months | 78.5 months | HR 0.86 (98% CI 0.55–1.34); P = 0.22 |
| Trial disposition | Stopped for futility at 75% information fraction |
3. Fovinaciclib halves progression risk in first-line HR+/HER2− advanced breast cancer — JAMA Oncology
| Endpoint | Fovinaciclib + AI | Placebo + AI | Result |
|---|---|---|---|
| Median PFS (BICR, primary) | Not reached | 20.2 months (95% CI 16.4–NE) | HR 0.55 (95% CI 0.38–0.77); P < 0.001 |
| Discontinuation due to TEAEs | 1.4% (3/208) | 1.4% (3/209) | No difference |
| OS data | Immature (40 events, 9.6%) | — | Not yet reportable |
| EORTC QLQ-C30 (QoL) | Similar longitudinal changes | — | No detriment |
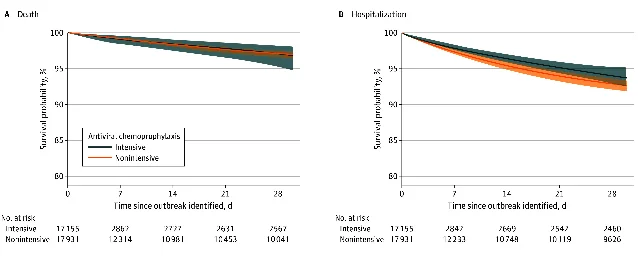
4. Intensive oseltamivir prophylaxis cuts 14-day hospitalization 21% in nursing home flu outbreaks — JAMA Internal Medicine
- Intensive strategy: oseltamivir chemoprophylaxis for ≥70% of eligible residents within 2 days of outbreak detection (including residents in non-affected units)
- Nonintensive strategy: 0% to <70% coverage within 2 days 7
| Endpoint | Intensive (≥70% coverage) | Nonintensive (<70% coverage) | Result |
|---|---|---|---|
| 14-day hospitalization | 3.58% | 4.54% | RR 0.79 (95% CI 0.64–0.96); RD −0.96% |
| 30-day hospitalization | 6.26% | 7.33% | Not statistically significant |
| 14-day all-cause death | 1.59% | 1.65% | RR 0.96 (95% CI 0.56–1.57); not significant |
| Sensitivity (≥80% coverage) | — | — | RR 0.74 (95% CI 0.59–0.91) |
5. Postdiagnostic statins cut breast cancer–specific mortality 32% in hormone receptor–positive subtypes — JAMA Network Open
| Endpoint | Statin users | Non-users | Result |
|---|---|---|---|
| Breast cancer–specific mortality (postdiagnostic use) | Lower | — | Age-adjusted HR 0.68 (95% CI 0.57–0.82) |
| All-cause mortality (postdiagnostic use) | Lower | — | HR 0.83 (95% CI 0.75–0.92) |
| Prediagnostic statin use | No association | — | Null result |
| Dose-response trend (postdiagnostic) | Present | — | Significant |
| Subtype specificity | HR+ subtypes (all 3) benefit; direction similar in TN | — | Consistent |
References
- 1Zenas BioPharma — INDIGO Phase 3 NEJM publication and EULAR 2026 presentation
- 2MedPage Today — Novel Biologic Performs Well in IgG4-Related Disease
- 3PubMed — INDIGO trial protocol (Culver et al., Rheumatol Ther 2026)
- 4PubMed — Adjuvant nivolumab vs observation in resected NSCLC (PMID 42224490)
- 5PubMed — Fovinaciclib for first-line therapy of advanced breast cancer (PMID 42224659)
- 6PubMed — Prompt and intensive antiviral chemoprophylaxis in nursing home influenza outbreaks (PMID 41910957)
- 7Infectious Disease Advisor — Intensive influenza prophylaxis in nursing homes reduces 14-day hospitalization risk
- 8PubMed — Statin use and survival in early breast cancer according to different intrinsic subtypes (PMID 42228366)
Add more perspectives or context around this Post.