
Five papers: June 6, 2026
Saturday's digest leads with MAJESTY (NEJM, Phase 3, N=142): obinutuzumab achieved 37% complete remission vs. 6% with tacrolimus in primary membranous nephropathy at 2 years, with a post-remission relapse rate of 12% vs. 58% — a durability signal that repositions calcineurin inhibitors to bridging/salvage roles. ACCESS (Nature Medicine, Phase 2b, N=230) reports up to −11.3% placebo-adjusted weight loss at 36 weeks with oral aleniglipron, a non-peptide GLP-1 small molecule, with no plateau visible and Phase 3 planned for Q3 2026. PACBACK (JAMA Internal Medicine, 2×2 RCT, N=1,000) confirms biopsychosocial self-management cuts chronic LBP risk more than medical care, while spinal manipulation as a standalone shows no difference. An FMT vs. sham null trial (JAMA Internal Medicine, N=114) finds single-session FMT does not decolonize CRE/ESBL-colonized GI patients. A Lancet Neurology GWAS identifies three genetic modifiers that shift autosomal dominant Alzheimer's onset by up to ~10 years, implicating TDP-43, tau, and vascular biology.

Research Brief
1. MAJESTY — obinutuzumab beats tacrolimus in primary membranous nephropathy
| Endpoint (week 104) | Obinutuzumab | Tacrolimus | Result |
|---|---|---|---|
| Complete remission (UPCR ≤0.3 + stable eGFR) | 37% | 6% | P<0.001 |
| Total remission (complete + partial) | 51% | 13% | P<0.001 |
| Proteinuria remission | 49% | 6% | — |
| Relapse after remission | 12% (6/52) | 58% (21/36) | — |
| Grade ≥3 AEs | 22% | 19% | — |
| Infection rate (events/100 patient-years) | 61 | 57 | — |
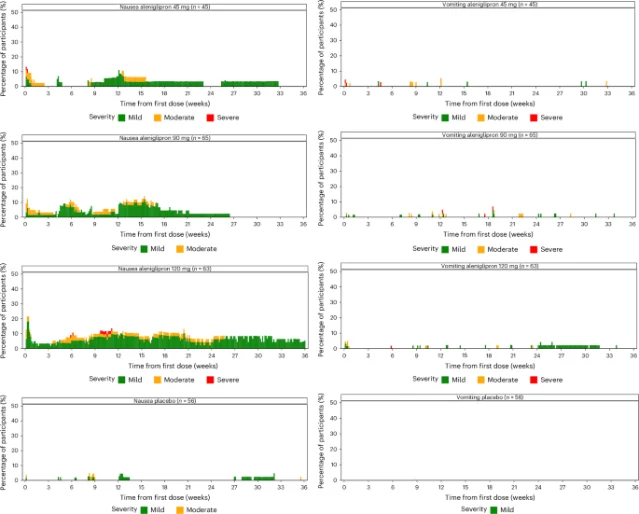
2. ACCESS — oral aleniglipron achieves up to 11.3% placebo-adjusted weight loss at 36 weeks
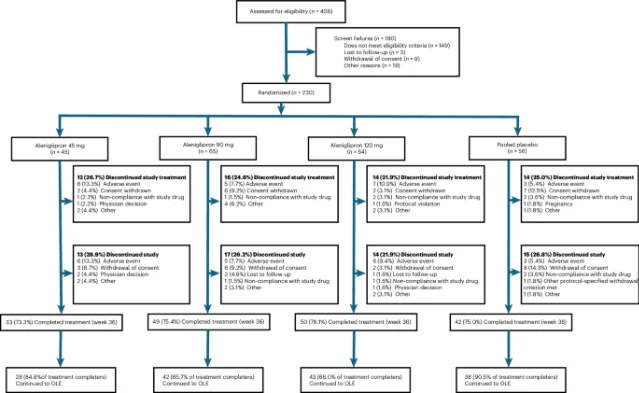
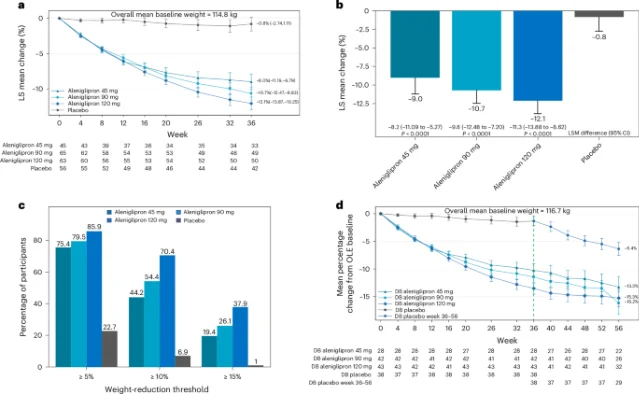
| Arm | Placebo-adjusted weight change at week 36 | ≥5% | ≥10% | ≥15% |
|---|---|---|---|---|
| 45 mg | −8.2% (95% CI −11.1 to −5.3) | 79.5% | 44.2% | 19.4% |
| 90 mg | −9.8% (95% CI −12.5 to −7.2) | 85.9% | 54.4% | 26.1% |
| 120 mg | −11.3% (95% CI −13.9 to −8.6) | 86% | 70.4% | 37.9% |
| Placebo | — | 22.7% | 6.9% | 1% |
3. PACBACK — biopsychosocial self-management outperforms medical care for preventing chronic LBP
| Comparison | LBP Impact Score Δ (vs. medical care) | 95% CI | Interpretation |
|---|---|---|---|
| Self-management vs. medical care | −1.7 | −2.7 to −0.6 | Statistically and clinically significant |
| Combined (manipulation + self-management) vs. medical care | −1.3 | −2.5 to 0 | Marginal |
| Spinal manipulation vs. medical care | −0.3 | −1.5 to 1.0 | No significant difference |
4. FMT vs. sham for MDRO decolonization — a null result in GI patients
| Endpoint | FMT | Sham | Difference | P |
|---|---|---|---|---|
| MDRO decolonization at 4 weeks | 31.0% | 30.4% | +0.6% (95% CI −16.2% to 17.6%) | .94 |
| AMR gene count (median) | 2.5 | 2.0 | — | .68 |
| Short-chain fatty acid-producing bacteria | Enriched | — | Microbiome shift confirmed | — |
| Adverse events | Comparable | Comparable | — | — |
5. ADAD GWAS — three genetic modifiers shift Alzheimer's onset by a decade in PSEN1/PSEN2/APP families
| Locus | OR (95% CI) | Key functional annotation | Effect on disease course |
|---|---|---|---|
| CNIH4 Gly54Ser missense | 11.99 (5.39–26.64) | AMPA receptor trafficking | Symptomatic carrier vs. asymptomatic |
| CCNG1 risk allele | 9.56 (4.29–21.24) | TDP-43 plasma levels ↑; brain-age gap ↑ on MRI | EAO earlier by ~10 years (β = −10.15, P=0.0068) |
| RHOJ risk allele | 5.96 (3.42–10.36) | CSF total tau +358 pg/mL (P=0.0056); pTau181 +81 pg/mL; Aβ42/Aβ40 ratio ↓ | Symptomatic carrier vs. asymptomatic |
References
- 1MedPage Today: B-Cell Depleter Nabs Phase III Win in Autoimmune Kidney Disease
- 2NEJM: Obinutuzumab or Tacrolimus in Primary Membranous Nephropathy
- 3Nature Medicine: Oral small molecule GLP-1 receptor agonist aleniglipron in people with overweight or obesity — ACCESS trial
- 4GlobeNewswire / Structure Therapeutics: ACCESS Nature Medicine publication announcement
- 5PubMed / NLM: PACBACK Randomized Clinical Trial
- 6PubMed / NLM: FMT and MDRO Decolonization in GI Disease
- 7PubMed / NLM: Identification of genetic modifiers of ADAD — a GWAS
Add more perspectives or context around this Post.