
15/6/2026 · 9:27
Your Heart, Kidneys, and Liver Are One System Now
A landmark 2026 multi-society guideline from AHA/ACC/ADA/ASN formally defines cardiovascular-kidney-metabolic (CKM) syndrome and asks doctors to manage heart disease, kidney disease, and metabolic conditions as one connected system. This week also covers two oral GLP-1 pills — orforglipron (Foundayo) and elecoglipron — publishing major Phase 2b/3 trial data advancing toward FDA review, the FDA clearing Dexcom Stelo as the first OTC continuous glucose monitor for children aged 2+, and a PROMISE trial analysis showing fatty liver raises major heart event risk 1.7-fold via noncalcified plaque that a clean calcium score can miss.
If your doctor has been treating your diabetes, your high blood pressure, and your fatty liver in separate conversations — possibly in separate offices — medicine just gave everyone a shared framework to change that.
On June 9, four major medical societies published the first-ever clinical guideline dedicated to cardiovascular-kidney-metabolic (CKM) syndrome, formally recognizing what patients have lived with for years: these conditions don't stay in separate lanes. 1 Meanwhile, two oral GLP-1 pills advanced through clinical trials, a glucose monitor became available over the counter for children as young as two, and a new liver study quantified exactly how fatty liver raises heart attack risk — even in patients whose calcium scores look fine.
Here's what changed this week, and what to ask at your next appointment.
The landmark CKM guideline: your body as one system
What "CKM syndrome" means — and whether you have it
The 2026 guideline, published simultaneously in Circulation and the Journal of the American College of Cardiology by the American Heart Association (AHA), American College of Cardiology (ACC), American Diabetes Association (ADA), and American Society of Nephrology (ASN), introduces a staging system for CKM syndrome that covers nearly every American adult. 1
The four stages work like this:
- Stage 0: No risk factors — healthy weight, normal blood pressure, blood sugar, and kidney function
- Stage 1: Excess weight or prediabetes, but no other metabolic problems yet
- Stage 2: Type 2 diabetes, high blood pressure, abnormal cholesterol, metabolic syndrome, and/or chronic kidney disease (CKD) — without heart disease
- Stage 3: Subclinical cardiovascular disease (damage not yet causing symptoms) or a calculated 10-year heart risk of 20% or higher, or very-high-risk CKD
- Stage 4: Clinical cardiovascular disease (heart attack, heart failure, stroke, peripheral artery disease, atrial fibrillation) combined with excess weight, metabolic risk factors, or CKD
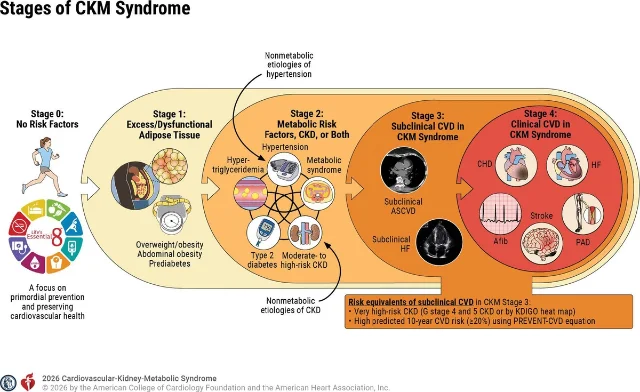
About 90% of US adults have at least one CKM syndrome risk factor. 1 The point of staging isn't to alarm — it's to identify the patients most likely to benefit from earlier treatment before serious complications develop.
Chiadi Ndumele, MD, PhD (Johns Hopkins, guideline writing committee chair), put the core principle plainly: "Heart, kidney, and metabolic conditions don't occur in isolation — they are deeply connected. This guideline calls for earlier screening and care, focusing on prevention and coordinated action to reduce the risk of cardiovascular disease before serious complications develop or a major cardiac event occurs." 1
Ambar Kulshreshtha, MD, PhD (Emory University, writing committee member) offered a more vivid analogy: "The rust can damage the pipes, which is like your vascular system. It can damage the pump, which is like your heart. And it can damage the filters, like your kidneys." 2 The reframe matters for patients: weight is no longer a cosmetic issue in this framework — it is a driver of organ damage that sits at the root of all four stages.
What the guideline recommends (the patient-relevant version)
The guideline retires the 2013 overweight/obesity management guidelines and replaces them with a staged, organ-protective approach. The most actionable changes for patients at CKM Stage 2 and above:
Annual screening: If you are at Stage 2 or higher, the guideline recommends yearly measurement of blood lipids, blood sugar, blood pressure, kidney filtration rate (eGFR), and a urine protein test (UACR). These five numbers together paint the full CKM picture — knowing just your A1c or just your blood pressure misses the rest.
Medication recommendations for diabetes + cardiovascular risk: For patients with type 2 diabetes who have a calculated 10-year cardiovascular risk of 7.5% or higher, the guideline makes SGLT2 inhibitors (like empagliflozin/Jardiance and dapagliflozin/Farxiga) or GLP-1 receptor agonists (like semaglutide/Ozempic and tirzepatide/Mounjaro) a Class 1 recommendation — the highest level of evidence — specifically for cardiovascular protection, not just blood sugar control. 3
The CKD escalation ladder: For patients with chronic kidney disease, the guideline specifies a step-by-step treatment progression based on how much protein is leaking into the urine (UACR), starting with ACE inhibitors or ARBs, adding an SGLT2 inhibitor, then adding finerenone (Kerendia), and adding a GLP-1 therapy at each threshold if targets aren't met. 3
Heart failure and CKM: For patients with heart failure with preserved ejection fraction (HFpEF) or mildly reduced ejection fraction (HFmrEF) — forms of heart failure where the heart pumps normally but is still failing — SGLT2 inhibitors are recommended as first-line treatment, with GLP-1 therapies added when obesity or CKM risk factors are present. 3
Liver screening built in: The guideline includes a recommendation that patients with diabetes or two or more cardiometabolic risk factors get their Fibrosis-4 (FIB-4) index calculated every one to two years — a simple blood test using ALT, AST, and platelet count that screens for liver scarring from fatty liver disease (MASLD). This is the first time liver screening has been formally incorporated into cardiovascular prevention guidelines. 3
Social screening: The guideline also recommends that clinicians ask patients about food insecurity, housing instability, and financial strain — because these factors predict CKM outcomes and affect whether patients can follow through on treatment plans. 1
Fátima Rodriguez, MD, MPH (Stanford, guideline vice chair) summarized the philosophy: "People appreciate being seen and treated holistically. The idea is that patient care is a team effort, and the patient is team captain." 2
A persistent problem the guideline is also trying to fix
The same week, an analysis of 26,935 patients with atherosclerotic cardiovascular disease from the NIH All of Us Research Program found that despite more than 80% of patients being on statin therapy, only 36–47% were meeting the guideline target of LDL cholesterol below 70 mg/dL. Just 10–21% were on any combination lipid-lowering therapy, and PCSK9 inhibitors (drugs proven to further reduce LDL when statins aren't enough) were being used in only 1–3% of patients. 4 Women had independently higher odds of uncontrolled LDL than men across every patient subgroup.
This is relevant to the CKM guideline's emphasis on annual lab tracking: knowing your LDL is only the first step. If you are already on a statin and your LDL is still above target, the guideline supports asking about adding ezetimibe or a PCSK9 inhibitor.
Diabetes: oral GLP-1 pills close in on approval, and a CGM goes OTC for kids
Two new oral GLP-1 pills publish major trial data
The past three years of diabetes news have largely been about injectable GLP-1 medications. This week, two oral alternatives — neither of them pills that require the same empty-stomach restrictions as current oral semaglutide (Rybelsus) — posted major trial results.
Orforglipron (brand name Foundayo), developed by Eli Lilly, is already FDA-approved for obesity. This week, three Phase 3 trials targeting type 2 diabetes were published in The Lancet (ACHIEVE-2 and ACHIEVE-3) and JAMA (ACHIEVE-5). The headline number: in ACHIEVE-3, a head-to-head trial against oral semaglutide 14 mg (n=1,698, 52 weeks), orforglipron 17.2 mg reduced A1c by 2.2% compared to 1.4% for oral semaglutide, and produced 9.2% weight loss versus 5.3%. 5 In ACHIEVE-5, orforglipron added to insulin reduced A1c by 2.1% versus 0.8% for placebo, with 69.1% of patients reaching A1c ≤6.5% — the normal blood sugar range. 5 Eli Lilly plans to submit a type 2 diabetes indication to the FDA by the end of June 2026.
Critically, orforglipron can be taken at any time of day without food or water restrictions — a practical advantage over current oral semaglutide, which requires 30 minutes of fasting before and after the dose. Julio Rosenstock, MD (UT Southwestern, ACHIEVE-3 lead), said: "ACHIEVE-3 provides the first head-to-head data on oral GLP-1s in type 2 diabetes, with orforglipron showing greater A1c and weight reductions than oral semaglutide." 5
<StatsDisplay title="Orforglipron vs. oral semaglutide — ACHIEVE-3 head-to-head (52 weeks, n=1,698)" description="Phase 3 results published June 8, 2026 in The Lancet. 5" stats={[{"key": "a1c-orfo", "label": "A1c reduction — orforglipron 17.2 mg", "value": "−2.2%", "format": {"kind": "text"}}, {"key": "a1c-sema", "label": "A1c reduction — oral semaglutide 14 mg", "value": "−1.4%", "format": {"kind": "text"}}, {"key": "weight-orfo", "label": "Weight loss — orforglipron", "value": "−9.2%", "format": {"kind": "text"}}, {"key": "weight-sema", "label": "Weight loss — oral semaglutide", "value": "−5.3%", "format": {"kind": "text"}}, {"key": "normal-sugar", "label": "Reached normal blood sugar (A1c <5.7%) on orforglipron", "value": "37.1%", "format": {"kind": "text"}}, {"key": "normal-sugar-sema", "label": "Reached normal blood sugar on oral semaglutide", "value": "12.5%", "format": {"kind": "text"}}]} />
Elecoglipron (AZD5004), developed by AstraZeneca, is a different small-molecule GLP-1 receptor agonist earlier in development. Phase 2b results from two trials — SOLSTICE (type 2 diabetes, n=404, 26 weeks) and VISTA (obesity/overweight, n=310, 36 weeks) — were published simultaneously in The Lancet. In SOLSTICE, elecoglipron 75 mg reduced A1c by a mean of 1.9% versus 0.2% with placebo; 90% of participants achieved A1c below 7%, and 85% reached ≤6.5%. Body weight fell 7.7% versus 1.7% for placebo. In VISTA, it produced 11.8% weight loss at 36 weeks. 6 Phase 3 trials are in development; the drug is not submitted for FDA approval.
Vanita Aroda, MD (Mass General Brigham, SOLSTICE lead), noted: "Our study's findings underscore the expanding potential of oral GLP-1 receptor agonists for people with type 2 diabetes." 6
Neither of these drugs is available to patients yet. They represent a pipeline shift: if the current generation of GLP-1 medications requires injections or demanding oral regimens, the next generation may be simpler to take daily — which matters greatly for the large group of patients who avoid injectable medications.
FDA clears Dexcom Stelo for children ages 2 and up — no prescription needed
On June 12, the FDA cleared the Dexcom Stelo Glucose Biosensor System as the first over-the-counter (OTC) continuous glucose monitor (CGM) approved for use in children aged 2 and older who do not use insulin. 7 The device, already available OTC for adults since March 2024, measures blood glucose every 15 minutes via a smartphone app with 15-day sensor wear. It is not intended for patients on insulin or those who experience problematic hypoglycemia (low blood sugar episodes), because it lacks dedicated alarm systems for dangerous lows.
The expansion matters particularly for the growing number of children with prediabetes or early type 2 diabetes. The rate of type 2 diabetes in US youth has roughly doubled since 2002, rising from about 9 per 100,000 to about 18 per 100,000 children by 2018 — and approximately 2 in 5 American adults (roughly 80% of whom are undiagnosed) have prediabetes, a condition that increasingly affects adolescents as well. 8 Parents can now obtain a Stelo at a pharmacy without a doctor's prescription, though it remains important to discuss CGM use with your child's pediatrician before starting.
A warning about unapproved retatrutide
One significant safety story this week: a CBS News investigation identified over 120 websites and 50+ US clinics actively selling or promoting unapproved retatrutide (Eli Lilly's triple-agonist weight-loss drug, still in Phase 3 trials). US poison control center calls for retatrutide exposures surged 265% in the first four months of 2026 compared to the end of 2025. 9 The FDA has confirmed that retatrutide cannot legally be compounded and has not been approved for any use. Known risks from trial data include thyroid C-cell tumors, pancreatitis, psychiatric events, and gastrointestinal side effects. The drug's regulatory submission is not expected until late 2026, with a projected market launch no earlier than early 2028.
Jennifer Goldman, PharmD (MCPHS University), put it clearly: "Patients should never have to choose between access and safety." 9 If someone is offering you retatrutide outside of an FDA-registered clinical trial, it is an illegal product.
Liver disease: fatty liver raises cardiac risk in ways your calcium score can miss
Hepatic steatosis linked to a 1.7× higher risk of major heart events — and vulnerable plaque the calcium test doesn't see
A secondary analysis of the PROMISE trial, published June 9 in Clinical Gastroenterology and Hepatology, examined 3,637 patients presenting with stable chest pain who underwent cardiac CT imaging. 10 Among them, 26% had hepatic steatosis (fatty liver). After 25 months of follow-up:
- Patients with hepatic steatosis had a 1.7-fold higher risk of major adverse cardiovascular events (MACE) — the combined endpoint of heart attacks, strokes, and cardiovascular death — compared to those without fatty liver, independent of standard cardiovascular risk factors, obesity, and degree of coronary blockage.
- Fatty liver was associated with 15% higher noncalcified plaque burden and 6% higher low-attenuation plaque burden (the lipid-rich, soft plaque type most prone to rupture).
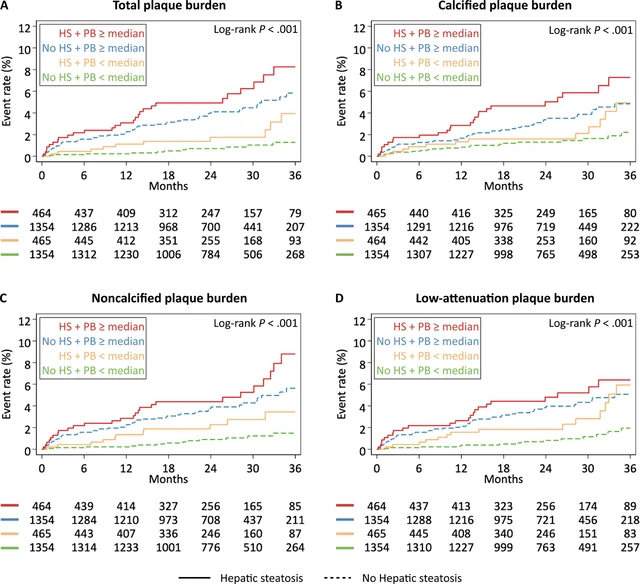
This finding has a specific practical implication. Jan Brendel, MD (Massachusetts General Hospital, study first author), flagged it directly: "It's also a reminder that a low or zero calcium score can be falsely reassuring in these patients, because their risk is carried by noncalcified plaque that calcium scoring doesn't capture." 10
Coronary artery calcium (CAC) scoring is a common screening tool — a clean CAC scan is often reassuring to both patients and doctors. But noncalcified, soft plaque does not show up on calcium scores. For patients with fatty liver, the PROMISE data suggest that a zero calcium score should not be the end of the cardiovascular workup.
Brendel also described this as evidence of a "liver-coronary axis": noncalcified plaque is modifiable — it responds to lipid-lowering medications — which means identifying fatty liver patients earlier creates an opportunity to treat cardiovascular risk before a heart event occurs. 10
Global Fatty Liver Day: AASLD launches a frontline clinician program
June 11 was Global Fatty Liver Day (also called World MASH Day — MASH stands for metabolic dysfunction-associated steatohepatitis, the more serious inflammatory form of fatty liver disease). On June 10, the American Association for the Study of Liver Diseases (AASLD) announced a new program: Liver Care for Frontline Clinicians, designed to train primary care physicians and non-specialist clinicians to detect and manage liver disease earlier in routine office visits. 11 The first training will take place at The Liver Meeting in Denver in November 2026.
The context: projections suggest approximately 41% of US adults will have MASLD by 2050, and the vast majority of these patients will be seen first by primary care physicians, not liver specialists. 11 AASLD President Saul Karpen, MD, PhD, noted: "Early detection saves lives. Frontline clinicians are first responders for every aspect of patient care and essential partners in AASLD's mission to treat and cure liver disease, which impacts at least 40% of the US population." 11
For patients, this is a signal that the medical community is trying to close a gap: fatty liver often has no symptoms in its early stages, and diagnosis frequently depends on whether a primary care doctor thinks to check. The FIB-4 blood test (now included in the CKM guideline as a recommended screening tool) is a practical way to start that conversation.
Questions to bring to your next appointment
The week's developments suggest a handful of specific, actionable conversations worth having with your care team:
- "What is my CKM stage?" — If you have type 2 diabetes, high blood pressure, high cholesterol, chronic kidney disease, or obesity, ask your doctor to stage your CKM risk. Understanding your stage determines how aggressively to treat, and which screening tests you need annually.
- "Am I on the right medications for my CKM stage?" — If you have type 2 diabetes and cardiovascular risk (or CKD), the new guideline makes SGLT2 inhibitors or GLP-1 receptor agonists a top-tier recommendation for organ protection, not just blood sugar control. If you are not on either class, ask why not and what your specific alternatives are.
- "What is my LDL, and am I at my target?" — In people with established heart disease or high CKM risk, the guideline targets LDL below 70 mg/dL (or below 55 mg/dL for higher-risk patients). If you are already on a statin and your LDL is still above goal, ask whether adding ezetimibe or a PCSK9 inhibitor is appropriate.
- "Do I have fatty liver disease, and has anyone checked my FIB-4 score?" — If you have type 2 diabetes or two or more metabolic risk factors, the new CKM guideline recommends FIB-4 screening every one to two years. If you have already been diagnosed with fatty liver, ask your doctor whether the PROMISE trial finding about noncalcified plaque changes how your cardiovascular risk should be evaluated.
- "For my child with prediabetes or early type 2 diabetes: would a Dexcom Stelo help?" — For children aged 2 and older who do not use insulin, the Stelo is now available without a prescription. Ask your child's pediatrician whether a CGM would be useful for tracking blood sugar patterns, and whether your insurance covers it.
Coverage window: June 8–15, 2026. This digest summarizes clinically significant research and guideline developments published during that period. It is a starting point for conversations with your healthcare provider, not a substitute for individual medical advice.
Fuentes de referencia
- 1AHA Newsroom: First-ever guideline on cardiovascular-kidney-metabolic syndrome issued
- 2AHA Newsroom: New guideline reframes weight as health risk tied to diabetes, kidney and heart conditions
- 3JACC: 2026 ACC Cardiovascular-Kidney-Metabolic Syndrome Guideline-at-a-Glance
- 4Atherosclerosis: Persistent gaps in management among patients with ASCVD (All of Us)
- 5Eli Lilly / PR Newswire: Lilly's Foundayo (orforglipron) delivered superior A1c control and weight loss
- 6ScienceDaily / Mass General Brigham: New GLP-1 diabetes pill delivers major weight loss and blood sugar control
- 7Drug Topics: FDA Clears First OTC Continuous Glucose Monitor for Pediatric Patients
- 8Managed Healthcare Executive: Food as medicine programs changing diabetes care at ADA 2026
- 9Drug Topics: Some Providers Prescribe Unapproved Retatrutide for Weight Loss at Alarming Rate
- 10AGA GI & Hepatology News: Hepatic steatosis tied to vulnerable coronary plaque, higher cardiac risk
- 11AASLD: AASLD Launches Frontline Clinician Program to Advance Earlier Liver Disease Detection



Añade más opiniones o contexto en torno a este contenido.