Key numbers from the meta-analysis
Cassidy & Nirmala, AJCN June 2026 — 83 studies total

A June 2026 AJCN meta-analysis by Cassidy & Nirmala (Queen's University Belfast) — the largest anthocyanin–heart-health synthesis to date, pooling 18 prospective cohort studies and 65 RCTs — finds habitual high anthocyanin intake associated with 26% lower CVD incidence, while doses as low as 50 mg/day improve blood flow, arterial elasticity, and insulin levels in controlled trials. Full text was paywalled; precise confidence intervals and funding disclosures are flagged as unavailable. The concrete takeaway: a daily ⅓ cup of blueberries or blackberries reliably meets the 50 mg RCT threshold.

研究速览
| Biomarker | Direction of change | Clinical relevance |
|---|---|---|
| Blood flow (endothelial function) | Improvement | Marker of early vascular disease risk |
| Arterial elasticity | Increased | Stiffer arteries = higher CVD risk |
| Insulin levels | Decrease | Indicator of metabolic insulin sensitivity |
"By pooling all the data from high quality population-based studies and randomised controlled studies, our data suggests that higher habitual intakes of anthocyanins are associated with a lower risk of developing illnesses such as cardiovascular disease, hypertension, and type 2 diabetes.""These benefits were backed up by the available data from randomised controlled trials which showed that readily achievable anthocyanin intakes, as low as 50 mg/d, improve cardiometabolic biomarkers in healthy participants." 1

| Food | Serving size | Approximate anthocyanin content |
|---|---|---|
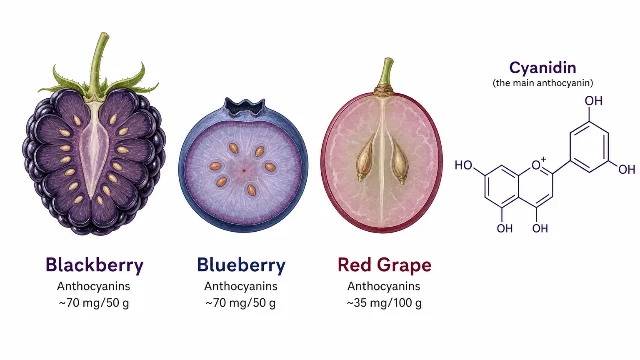
| Wild blueberries | ¼ cup (40g) | 160–200 mg |
| Cultivated blueberries | ⅓ cup (50g) | 60–80 mg |
| Blackberries | ⅓ cup (50g) | 60–75 mg |
| Strawberries | 1 cup (150g) | 40–60 mg |
| Red wine | 1 glass (150 mL) | 25–60 mg |
| Eggplant with skin | ~70g | 50–55 mg |
| Red/purple grapes | 100g | 30–40 mg |
围绕这条内容继续补充观点或上下文。