
Allulose vs. tagatose: a 20-trial meta-analysis finds both cut post-meal glucose spikes — but only tagatose lowers HbA1c
A 2026 systematic review and meta-analysis in The American Journal of Clinical Nutrition (Osborn et al.; 20 controlled trials, 1,033 adults) finds that both allulose and tagatose significantly reduce post-meal blood glucose and insulin spikes with moderate GRADE certainty. The key differentiator: tagatose also reduced HbA1c by 0.25 percentage points (95% CI −0.44 to −0.06; moderate certainty), a signal absent in allulose's 12-trial pool. Neither sweetener affected body weight, lipids, or body composition. Allulose is the practical default for reducing post-meal spikes; tagatose has the edge for long-term glycemic control. Actionable recommendation: swap table sugar for 1–2 teaspoons of allulose daily, or tagatose if sourcing it is feasible.

研究速览
Full-text note: The Osborn et al. 2026 AJCN paper is open-access by copyright (© 2026 The Author(s)) but remained behind publisher paywall/bot detection at the time of writing. All effect sizes below come from the PubMed structured abstract, Semantic Scholar record, and the Examine.com study summary. Per-study characteristics, forest plots, dose-response sub-analyses, and the complete GRADE summary table are unavailable until the full text is freely accessible.
What this study did and who it included
Allulose: reliable post-meal effect, silent on HbA1c
- Postprandial glucose incremental area under the curve (iAUC): SMD = −0.66 (95% CI −0.92, −0.39), moderate GRADE certainty 1
- Postprandial insulin: SMD = −1.27 (95% CI −2.14, −0.40), I² = 96%, p = 0.03, moderate GRADE certainty 1
Tagatose: larger glucose effect, a leaner insulin response, and the HbA1c edge
- Postprandial glucose iAUC: SMD = −1.03 (95% CI −1.36, −0.71), moderate GRADE certainty 1
- Postprandial insulin: SMD = −1.05 (95% CI −1.61, −0.49), moderate GRADE certainty 1
- HbA1c: MD = −0.25 percentage points (95% CI −0.44, −0.06), moderate GRADE certainty — the key differentiator 1
- Fasting insulin: MD = −80.40 pmol/L (95% CI −136.96, −23.84), very low GRADE certainty — interpret with caution 1

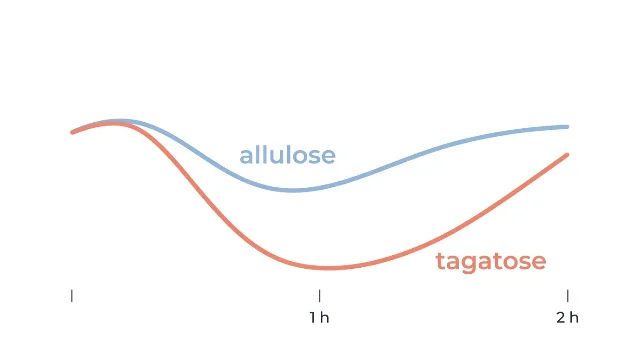
The shape of the glucose response
How these two sweeteners compare, head-to-head
| Feature | Allulose | Tagatose |
|---|---|---|
| Post-meal glucose reduction (SMD) | −0.66 (moderate certainty) | −1.03 (moderate certainty) |
| Post-meal insulin reduction (SMD) | −1.27 / I²=96% (moderate certainty) | −1.05 (moderate certainty) |
| HbA1c reduction | No significant effect | −0.25% (moderate certainty) |
| Sweetness vs. sucrose | ~70% | ~92% |
| Calories | 0.4 kcal/g | 1.5 kcal/g |
| Glycemic index | ~0 | ~3 |
| Single-dose GI tolerance limit | ~28 g (~7 tsp) | ~30 g (~7.5 tsp) |
| Daily upper limit | ~60 g (~15 tsp) | ~30–45 g (estimated) |
| US label treatment | Excluded from Added Sugars | Counts as Added Sugars |
| Prebiotic benefit | Not established | Yes — Bifidobacterium support |
| US retail availability | Widely available (Truvia, Wholesome, RxSugar) | Limited (Amazon, specialty retailers) |
| Cost per kg (approx.) | ~$6–10 | ~$10–18 |

How this fits the prior evidence
Limitations and what remains unknown
What this is — and what it isn't — from the author's perspective
The concrete recommendation
参考来源
- 1Osborn et al. 2026 — AJCN (PubMed structured record, PMID 41985675)
- 2BYU Life Sciences: Lauryn Osborn rare sugars feature
- 3Examine.com study summary — Osborn et al. 2026
- 4Icon Foods: Tagatose v. Allulose for food and beverage formulators
- 5GreyB: Allulose vs. Tagatose market analysis
- 6Semantic Scholar record — Osborn et al. 2026 (prior SR references)
- 7NutritionFacts.org: Does allulose have side effects? (Dr. Michael Greger)
围绕这条内容继续补充观点或上下文。