Krill oil outpaces fish oil for plasma omega-3
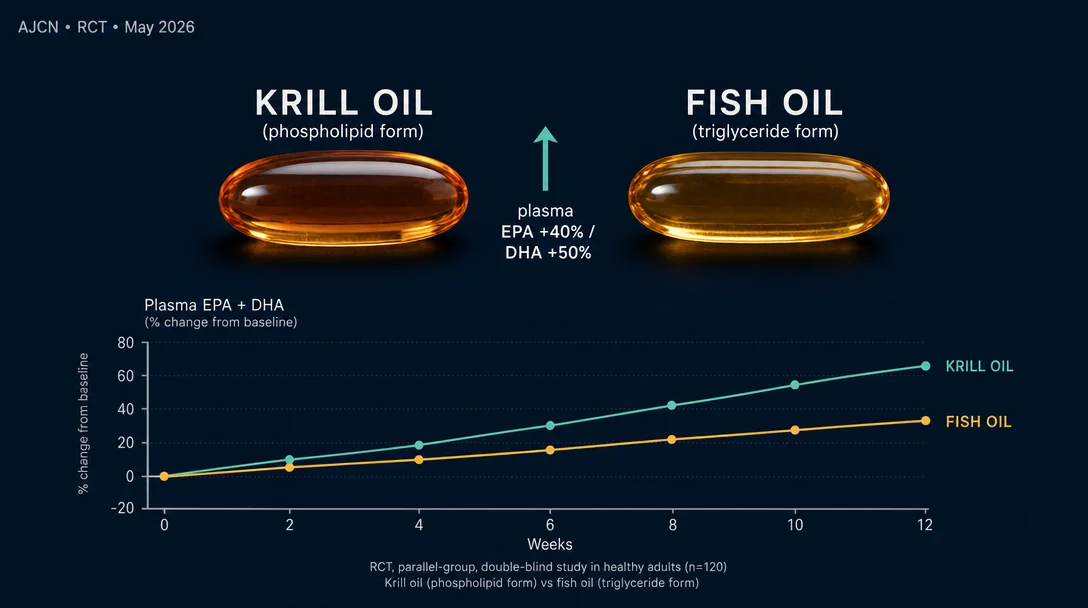
A double-blind RCT in AJCN (May 16, 2026) found that krill oil delivers 1.4× more plasma EPA and 1.5× more plasma DHA than fish oil at the same 1.1 g/day dose over 12 weeks — meaning the two supplements are not dose-for-dose interchangeable.

研究速览
When researchers gave healthy adults the same daily amount of omega-3 from two different sources, the molecular packaging turned out to matter. A double-blind randomized controlled trial published May 16, 2026 in The American Journal of Clinical Nutrition found that krill oil produced plasma EPA levels 1.4 times higher and plasma DHA levels 1.5 times higher than fish oil after 12 weeks — at an identical 1.1 g/day omega-3 dose. 1
The difference comes down to molecular form. Krill oil delivers EPA and DHA bound to phospholipids (primarily phosphatidylcholine). Fish oil delivers them as triglycerides or ethyl esters. That structural distinction, the study suggests, is not pharmacologically trivial.
Note: The full text of this paper is behind the AJCN paywall. All numerical data below come from the published abstract and trial registration record (NCT04279743). Funding sources and the complete author list are not yet publicly available.
What the study did
The trial, led by I. Loukil and colleagues (trial registration: NCT04279743, published as a Journal Pre-proof), enrolled 72 healthy adults and randomized them into two parallel arms: 1
- Krill oil group (n=36): 1.1 g/day omega-3 as phospholipid-bound EPA+DHA
- Fish oil group (n=36): 1.1 g/day omega-3 as triglyceride-form EPA+DHA
Participants were matched by age and BMI. The sample skewed female: 53 women and 19 men. Both groups took their supplements daily for 12 weeks under double-blind conditions — neither participants nor researchers knew which supplement was being taken.
Blood draws happened at baseline and at weeks 1, 2, 4, and 12. Plasma fatty acid concentrations were quantified by gas chromatography–flame ionization detection (GC-FID), a standard analytical method for plasma lipid profiling. The weekly sampling schedule allowed the researchers to track not just the endpoint result, but how the plasma enrichment curve developed over time — an important design choice that separates this study from earlier single-timepoint comparisons.
The study's primary statistical test was a time × treatment interaction, asking whether the two supplements produced diverging plasma trajectories rather than a simple end-of-study difference.
What the blood data showed
Both supplements raised plasma EPA and DHA above baseline. Krill oil raised them more — and the gap widened as the weeks progressed. 1
| Outcome | Time × treatment interaction | Krill oil advantage at week 12 |
|---|---|---|
| Plasma EPA (Δ from baseline) | p = 0.0001 | 1.4× greater than fish oil |
| Plasma DHA (Δ from baseline) | p = 0.005 | 1.5× greater than fish oil |
The p-values here reflect the overall trajectory divergence, not a single endpoint comparison — meaning krill oil's advantage was consistent across the measurement timepoints, not a fluctuation at week 12 alone.
Sex modified the EPA response. A significant time × sex interaction (p = 0.026) showed that women's plasma EPA rose 1.5 times more than men's over the 12 weeks. This interaction was specific to EPA; DHA did not show a statistically significant sex difference. 1 Whether this reflects a hormonal modulation of phospholipid absorption, differences in baseline fatty acid metabolism, or simply the sample's sex imbalance (53 women vs. 19 men) cannot be determined from the abstract alone.
The study also examined the APOE4 (apolipoprotein E ε4) genotype, which is associated with altered lipid metabolism and elevated Alzheimer's disease risk. APOE4 carriers showed approximately 3× baseline elevation in EPA and 1.6× in DHA, regardless of which supplement they took. 1 However, there was no statistically significant genotype × treatment interaction — meaning the krill oil advantage held equally regardless of APOE4 status. The authors conclude that krill oil outperforms fish oil "regardless of APOE4 genotype."
How this fits prior work
The idea that phospholipid-bound omega-3s absorb more readily than triglyceride forms is not new, but the evidence base has been inconsistent. A 2015 study by Köhler and colleagues (PMC4374210) found that krill oil produced a significantly higher acute EPA+DHA area under the curve (AUC) compared to fish oil triglycerides and ethyl esters in a postprandial absorption test — a single-dose pharmacokinetic comparison. 2 A 2020 study published in MDPI Nutrients (Sung et al.) found that krill oil and fish oil produced different plasma lipidome profiles after 30 days, but the differences were not uniformly in krill oil's favor. 2
Where the Loukil 2026 trial adds something neither of those could: a dose-matched, double-blind, 12-week parallel design with weekly blood sampling. Acute AUC studies capture a single absorption event; 30-day studies may not reach steady state. A 12-week study with matched doses measures the clinically relevant question — whether the phospholipid form confers a sustained plasma advantage under conditions that resemble realistic supplementation.
The direction of the evidence is consistent (phospholipid form appears better absorbed), but the Loukil study is the cleanest test of this question to date at this timescale.
What the study cannot tell you
Several limitations apply before drawing clinical conclusions.
Sample size and population: With 36 participants per arm, the trial is adequately powered to detect a sustained time × treatment effect, but subgroup analyses — particularly the APOE4 and sex findings — carry wider uncertainty intervals. The population was healthy adults, which limits direct extrapolation to people with metabolic disease, cardiovascular disease, or malabsorption conditions.
No hard clinical endpoints: The study measured plasma EPA and DHA as its outcome. Higher plasma omega-3 levels are associated with reduced cardiovascular and inflammatory disease risk in observational research, but this trial did not measure whether the plasma advantage translated into any clinical outcome difference. The assumption that more plasma EPA/DHA is better is biologically plausible, not directly tested here.
Exact EPA and DHA milligrams per supplement not disclosed in the abstract: The total omega-3 dose was 1.1 g/day, but the specific EPA:DHA ratios in each supplement are not reported in the publicly available text. If the two products had meaningfully different EPA:DHA ratios at the same total omega-3 dose, that could partly confound the comparison.
Full text inaccessible: Funding sources and conflict-of-interest disclosures were not retrievable from the abstract. Krill oil is a commercially significant ingredient, and research in this space has a history of industry involvement. These declarations matter for interpreting effect sizes.
Duration: 12 weeks is adequate for reaching steady-state plasma levels, but long-term effects beyond three months are unknown from this study.
The dietary decision
The practical implication of this finding is about dose equivalence, not just product preference.
If you currently take a fish oil supplement for omega-3 benefits, the Loukil RCT suggests that an equal dose of krill oil will produce meaningfully higher plasma EPA and DHA — specifically, roughly 40% more EPA and 50% more DHA at steady state. Stated differently: to reach the plasma omega-3 level that 1.1 g/day of krill oil produces, fish oil users would need a higher daily dose.
For health-conscious adults and clinicians advising on supplementation, here is what the evidence supports today:
If you are considering starting or switching omega-3 supplements: Krill oil at the same labeled omega-3 dose as your current fish oil appears to deliver greater plasma enrichment. The phospholipid form matters biologically, and the 12-week sustained advantage in this RCT is not a single acute absorption fluke.
If you are a woman supplementing for cardiovascular or inflammatory reasons: The sex-stratified EPA finding (women's EPA response 1.5× men's) suggests women may see an amplified benefit from the phospholipid form specifically on EPA. This remains a subgroup result from a 53-woman sample, so caution in overstating it is warranted — but the direction is worth tracking as larger trials emerge.
If your goal is achieving a target plasma EPA+DHA level: The dose-matching logic here is directly actionable. A lower krill oil dose may be sufficient to reach the same plasma target as a higher fish oil dose. For patients where supplement cost or pill burden is a consideration, this is a relevant trade-off to discuss.
One practical caveat: Krill oil is more expensive per gram of omega-3 than fish oil. Whether the plasma advantage justifies the price difference is a personal and clinical calculation, not a finding this study resolves. What the study does resolve is that the two products are not dose-for-dose interchangeable.
The authors' own conclusion from the abstract is direct: "Individuals with higher ω-3 FA requirements may achieve adequate enrichment with lower doses of krill oil compared to fish oil supplementation." 1 That is a claim worth watching as the full text becomes accessible and independent replication follows.
围绕这条内容继续补充观点或上下文。