

www.nature.com
Time-restricted eating and cardiometabolic health in community-dwelling adults — Feit et al. 2026, EJCN
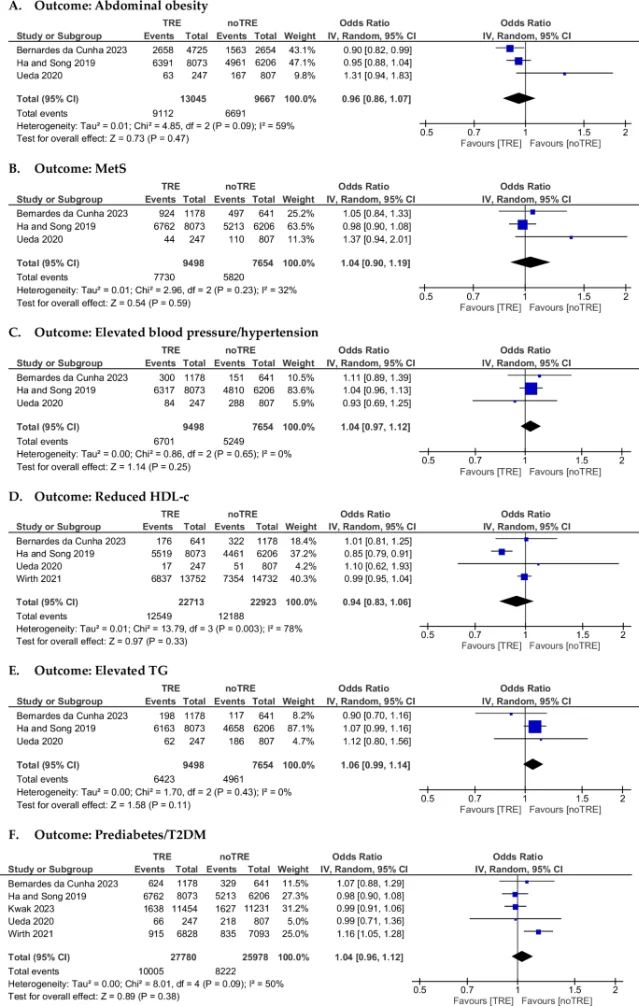
First SR/MA of observational studies on TRE and cardiometabolic health. Six meta-analyses across 18 studies; all pooled ORs crossed 1.0. Open access, CC BY 4.0.
围绕这条内容继续补充观点或上下文。