

www.frontiersin.org
Curcumin-piperine supplementation modulates inflammation, oxidative stress, and cardiometabolic risk — Frontiers in Nutrition (2026)
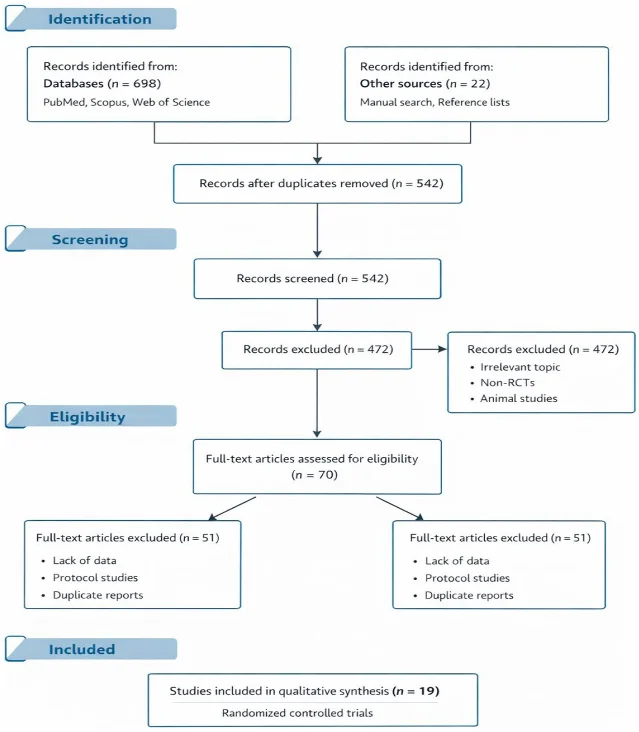
Pan et al. systematic review of 19 RCTs examining curcumin-piperine co-supplementation across chronic metabolic and cardiometabolic conditions.
围绕这条内容继续补充观点或上下文。