Vitamin D does not improve lung function in children with asthma
A 2026 systematic review and meta-analysis of 12 RCTs (1,239 children aged 4–18) found vitamin D supplementation produces no significant improvement in lung function, airway inflammation, or asthma control scores. The key distinction: vitamin D may reduce acute exacerbations in deficient children, but should not be used as a tool for improving stable lung function.

研究速览
A new meta-analysis of 12 randomized controlled trials finds no benefit of vitamin D supplementation on breathing capacity, airway inflammation, or day-to-day asthma control in children with asthma. The finding matters because vitamin D supplements are already part of many pediatric asthma management plans — often based on the assumption that correcting deficiency will improve overall respiratory health. This paper draws a harder boundary around what the vitamin actually does.
The study was published May 19, 2026 in Frontiers in Nutrition (Nutritional Immunology section). 1
What the meta-analysis found
Li and colleagues pooled 12 RCTs involving 1,239 children ages 4–18 with physician-diagnosed asthma, all comparing oral vitamin D supplementation to placebo. 1 The results across every outcome measured were null:
- FEV1 (forced expiratory volume in one second — the standard measure of airflow obstruction): no statistically significant improvement
- FVC (forced vital capacity): no significant improvement
- FEV1/FVC ratio: no significant improvement
- PEF (peak expiratory flow): no significant improvement
- FeNO (fractional exhaled nitric oxide, a marker of airway inflammation): no significant change
- cACT score (childhood Asthma Control Test): no significant improvement
- IgE (serum total immunoglobulin E, an allergic marker): no significant change
The authors' conclusion is direct: "Overall, the current evidence does not support the routine use of vitamin D supplementation to improve lung function in children with asthma." 1
Study design and population
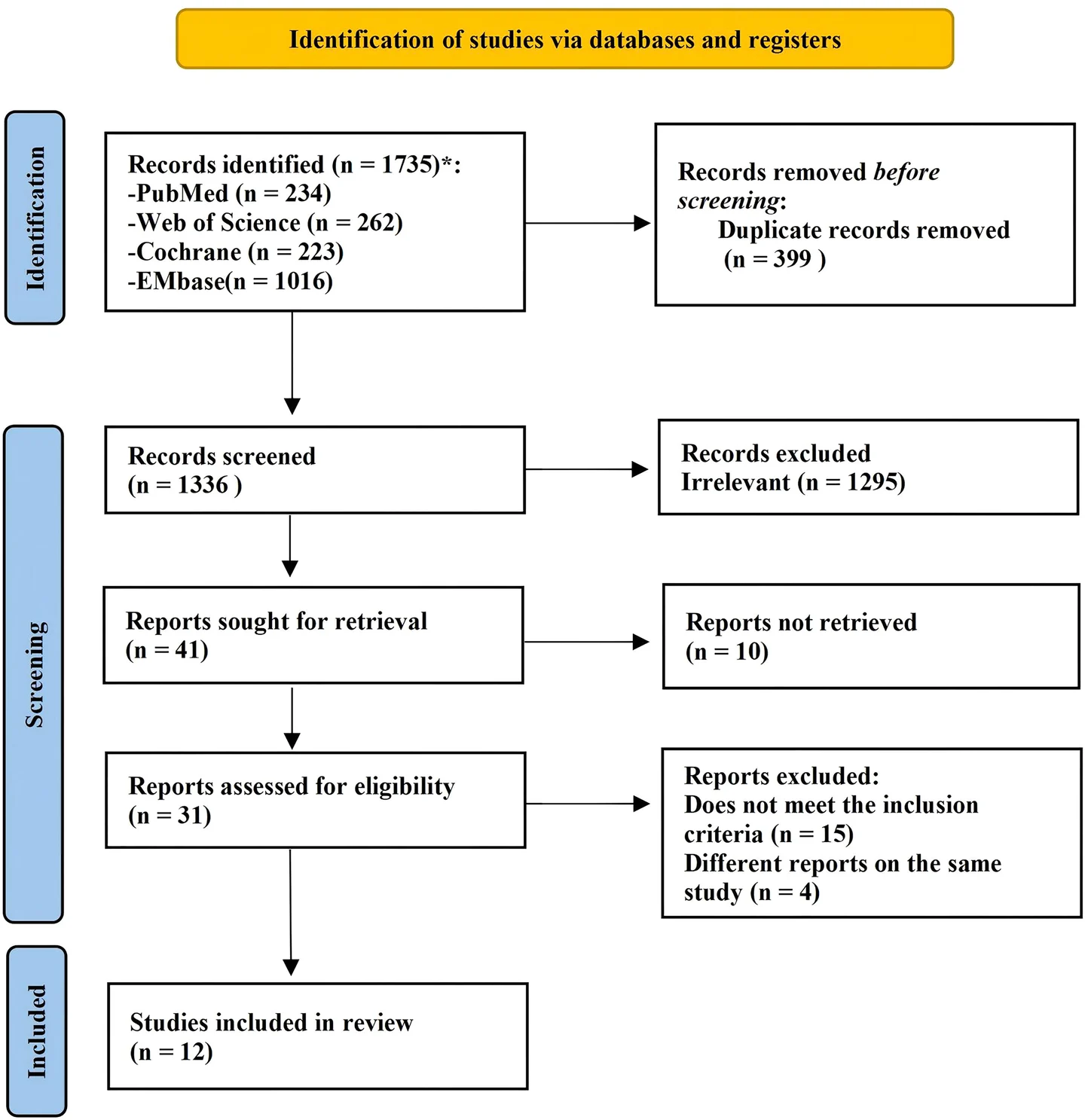
The systematic review and meta-analysis searched four databases (PubMed, Web of Science, Embase, Cochrane Library) through October 31, 2025. 1 From 1,735 records, 12 trials met inclusion criteria. The study was prospectively registered with PROSPERO (CRD420251270660). 2
The 12 included trials spanned 9 countries — India (2), China (2), Poland (2), Japan, Pakistan, Israel, the United States, Ireland, and Turkey — giving the dataset reasonable geographic breadth. Vitamin D doses ranged from 500 to 4,000 IU/day; the majority of trials (6 out of 12) used doses under 1,000 IU/day. Study duration ranged from 9 days to 12 months. All interventions used oral supplements, predominantly vitamin D3 (cholecalciferol).
All five authors are from the Department of Pediatrics at Shengjing Hospital of China Medical University, Shenyang, China. The study received funding from the National Natural Science Foundation of China and the National Health Commission; no conflicts of interest were declared.
Figure from: Li R et al. (2026), Frontiers in Nutrition
Risk of bias was assessed using the Cochrane ROB 2.0 tool. Six of 12 studies were rated low risk overall; 3 had some concerns (primarily around unclear allocation concealment or pre-specified analysis plans); 3 were rated high risk, chiefly because of missing outcome data. 1
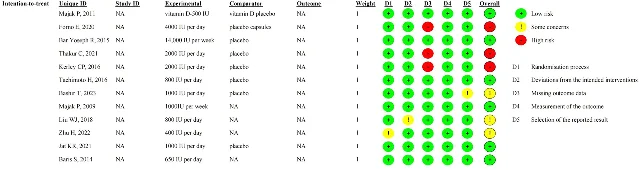
Figure from: Li R et al. (2026), Frontiers in Nutrition
The numbers — what changed and what didn't
FEV1 was the primary outcome, analyzed from 9 of the 11 trials that reported lung function data (838 participants; 420 vitamin D, 418 placebo). The pooled standardized mean difference was SMD 0.39 (95% CI −0.13 to 0.92). 1 The confidence interval crosses zero, meaning no statistically significant benefit. Heterogeneity was very high: I²=92% (P<0.0001). The change-from-baseline analysis told the same story: SMD 0.21 (95% CI −0.64 to 1.06, I²=91%).
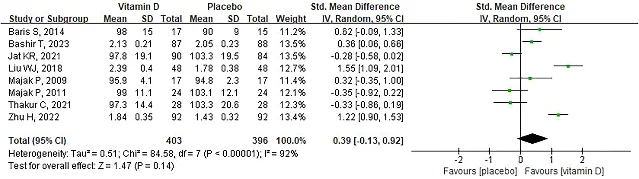
Figure from: Li R et al. (2026), Frontiers in Nutrition
A sensitivity analysis removing one study at a time confirmed that no single trial was driving the null result. Publication bias testing via Egger's test returned P=0.922, which does not indicate significant bias — though with fewer than 10 studies contributing to some analyses, this test has limited power. 1
The cACT score (childhood Asthma Control Test, a validated seven-item questionnaire scored 0–27, with higher scores indicating better control) was the most consistent null result: MD 0.16 (95% CI −0.55 to 0.88), I²=0% across 3 studies. 1 Zero heterogeneity means the three contributing trials agreed with each other — vitamin D moved the asthma control needle by essentially nothing.
IgE (serum total IgE, an indicator of allergic sensitization) also showed a consistent null: SMD −0.14 (95% CI −0.61 to 0.33, I²=0%). 1
The authors did conduct exploratory subgroup analyses by dose (<1,000 IU/day, 1,000 IU/day, 2,000 IU/day), duration (9 days, ≤3 months, >3 months), baseline vitamin D status, and corticosteroid co-use. One subgroup signal appeared: the <1,000 IU/day dose group showed a borderline-significant FEV1 improvement (SMD 0.70, 95% CI 0.04–1.36, I²=88%). 1 One duration-based outlier also appeared: a single 9-day trial (Liu 2018, n=96, severe asthma, 800 IU/day with glucocorticoids) showed a significant FEV1 improvement (SMD 1.55, 95% CI 1.09–2.01). The authors are explicit that these analyses "should be regarded as exploratory" — they were not pre-registered, were defined post-hoc, and individual subgroups involved small sample sizes with high heterogeneity.
The exacerbation exception
This null result applies specifically to stable, day-to-day respiratory parameters. A separate line of evidence addresses a different question: does vitamin D reduce how often acute asthma attacks occur?
Two earlier meta-analyses point in a different direction. Fedora et al. (2024) in Annals of Medicine found that standard-dose vitamin D significantly reduces asthma exacerbation frequency in children — but, critically, that meta-analysis also found no improvement in FEV1. 3 Liu et al. (2022) in Frontiers in Nutrition reached the same dual conclusion. 4 The two bodies of evidence point in consistent directions: vitamin D appears to reduce attack frequency, but does not improve baseline lung mechanics.
The authors of the current paper frame this as a biologically meaningful distinction. Vitamin D's immunomodulatory effects may operate through reducing the inflammatory cascade triggered during acute episodes (cathelicidin, interleukin-10, regulatory T-cell pathways), while the structural determinants of baseline airflow — airway remodeling, smooth muscle tone, mucus production — may not respond to vitamin D on the timescales and doses tested. They also invoke the Heaney framework for nutrient sufficiency: vitamin D supplementation is "most likely to confer benefits when individuals are in a deficient state, whereas the incremental benefits of further increasing intake once sufficiency has been achieved may be attenuated." 1
In other words: correcting deficiency may provide the exacerbation benefit. Supplementing a child who is already vitamin D sufficient probably does not further improve their lungs.
Limitations
Several constraints on interpreting these results deserve explicit attention.
Heterogeneity. I² exceeded 90% for FEV1, FVC, and FEV1/FVC — values that high indicate the pooled estimate should be interpreted with caution. The authors attribute it to differences in baseline asthma severity, co-medications, vitamin D dosing, and lung function measurement methods, but they could only run subgroup analyses for FEV1 (not secondary outcomes) due to the limited number of studies. 1
Study quality. Three of 12 included trials were rated high risk of bias, primarily because of missing outcome data. Excluding these would reduce the dataset further.
Population. Most participants had baseline FEV1 >80% predicted, meaning the enrolled children had mild-to-moderate asthma at most. Results may not apply to children with severe airflow limitation. The prior Liu 2022 meta-analysis suggested vitamin D might benefit patients with FEV1 <70%, but the current data cannot test that threshold. Seven of 12 studies were conducted in Asian populations, where baseline vitamin D insufficiency or deficiency was common — the generalizability to populations with higher baseline vitamin D status is uncertain.
Surrogate endpoints. FEV1 is a surrogate endpoint. It is strongly associated with asthma outcomes in clinical research, but the COMSA (Core Outcome Measure Set for Asthma) recommends measuring exacerbation rate, oral corticosteroid use, quality of life (PAQLQ), and ACT score as primary outcomes for pediatric severe asthma — most of which were rarely reported in the included trials. 1
Subgroup analyses. The dose-based and duration-based subgroup hints described above were post-hoc and not pre-registered with PROSPERO. They should not be used as a basis for clinical dosing recommendations without replication in prospective trials.
The dietary takeaway
The evidence now supports a clear, risk-stratified framework for vitamin D in childhood asthma:
Do not supplement vitamin D expecting it to improve your child's lung function, airway inflammation, or asthma control scores. The best-quality evidence to date — 12 RCTs, 1,239 children — finds no effect on any of these parameters. If a clinician or product is recommending vitamin D on the basis that it will improve FEV1 or reduce FeNO, the current evidence does not support that specific claim.
Vitamin D may still be worth discussing for children who have frequent acute asthma attacks and who are vitamin D deficient. Prior meta-analyses consistently find a reduction in exacerbation frequency with supplementation. That benefit is most plausible in deficient children — checking serum 25-hydroxyvitamin D (25(OH)D) before supplementing is a more defensible approach than routine supplementation across all asthmatic children.
For dietitians advising families: The strongest dietary signal here is to ensure adequate vitamin D status through diet and sun exposure as a baseline for general pediatric health — not as an asthma-specific intervention. Food sources (fatty fish, fortified dairy, fortified plant-based milks, egg yolks) contribute modestly to serum levels, and deficiency correction may matter more than high-dose supplementation above sufficiency.
For parents of asthmatic children: If your child already has confirmed vitamin D sufficiency (serum 25(OH)D ≥50 nmol/L — one widely used threshold; clinical cut-offs vary by lab), adding a vitamin D supplement for asthma management is not well-supported by current RCT evidence. If your child has recurrent acute episodes and has not had their vitamin D status tested, that assessment is worth raising with their clinician — not because supplementation will clear up their lung function, but because deficiency correction may reduce how often attacks occur.
The distinction between stable breathing capacity and acute attack frequency is the actionable takeaway from this meta-analysis. Vitamin D is not a bronchodilator. It may be a mild exacerbation buffer — and only in the right patient.
Cover image from: Li R et al. (2026), Frontiers in Nutrition
参考来源
- 1The efficacy of vitamin D supplementation in the management of childhood asthma: a systematic review and meta-analysis
- 2PROSPERO Registration CRD420251270660
- 3Vitamin D supplementation decrease asthma exacerbations in children: a systematic review and meta-analysis of randomized controlled trials
- 4A Meta-Analysis on Vitamin D Supplementation and Asthma Treatment
围绕这条内容继续补充观点或上下文。