
A 5-day fasting kit lowered blood sugar and LDL — but gains vanished within a month
A June 2026 RCT in Genome Medicine (n=64) found that five days on a 623 kcal/day plant-based fasting kit produced significant drops in blood glucose and LDL-cholesterol — but all metabolic benefits returned to baseline within one month. Seven of twelve authors are employed by the kit's manufacturer.

研究速览
A new randomized controlled trial (RCT) tested an at-home modified fasting kit against a habitual-diet control. The short answer: the metabolic improvements were real. The longer answer: they were almost entirely gone four weeks later — and the blood pressure benefits that circulated in the preprint turned out not to survive peer-review corrections. 1
What was tested
Researchers at the Buchinger Wilhelmi clinic in Überlingen, Germany, randomized 64 healthy adults (32 per arm, 22 men / 42 women, ages 18–80) to either five days on a pre-packaged plant-based fasting kit — the Buchinger Wilhelmi FASTING BOX — or their usual diet, followed by four days of gradual food reintroduction. Blood and stool samples were collected at baseline (T0), the end of fasting (T1, day 6), the end of reintroduction (T2, day 10), and one month later (T3). 1
The kit provides an average of 623 kcal/day — roughly a third of a typical adult's intake. Its macronutrient split is heavily fat-forward: 64.7% of calories from fat (primarily flaxseed and algae oil), 26.6% from carbohydrates, and just 6.2% from protein (about 9.8 g/day). The result is a ketogenic-range composition with minimal protein. Participants drank at least 2.5 liters of water or herbal tea daily. The prepackaged 24-ingredient kit includes vegetable broth, hummus, apple puree, honey, cashews, and a mineral supplement (calcium, potassium, magnesium, and zinc citrate). 1
The study is registered as NCT05821660 ("Fastreset") on ClinicalTrials.gov. 2
What the numbers showed
The panel of metabolic changes measured at the end of the 5-day fast (T1) and after reintroduction (T2) looked like this:
| Outcome | Timing | MFP group change | Control group change | p-value |
|---|---|---|---|---|
| Body weight | T1 (end of fast) | −3.1 kg (raw) | −0.15 kg | <0.001 |
| Blood glucose | T1 | −0.75 mmol/L | +0.19 mmol/L | <0.001 (net diff: −0.94) |
| Systolic BP | T1 | −0.75 mmHg | −0.03 mmHg | 0.08 (NS) |
| Diastolic BP | T1 | −0.67 mmHg | −0.21 mmHg | 0.13 (NS) |
| Systolic BP | T2 (post-reintro) | −0.56 mmHg | −0.16 mmHg | 0.046 |
| Diastolic BP | T2 | −0.36 mmHg | −0.01 mmHg | 0.007 |
| Total cholesterol | T2 | −0.74 mmol/L | −0.23 mmol/L | <0.001 |
| LDL-cholesterol | T2 | −0.63 mmol/L | −0.11 mmol/L | <0.001 |
| Uric acid | T1 | +143.68 µmol/L | −3.53 µmol/L | <0.001 |
The glucose signal is the cleanest: the MFP group fell 0.75 mmol/L while the control group rose 0.19 mmol/L, a net intergroup difference of 0.94 mmol/L (~17 mg/dL). 1
The LDL and cholesterol reductions are notable but show up only after the 4-day food reintroduction, not during the fast itself — suggesting the rebound diet matters as much as the fast.
Blood pressure did reach significance at T2 (after reintroduction) but not at T1 (end of fasting). That gap matters clinically: if someone expects an acute blood pressure drop from a week of fasting, this trial does not support it.
The elevation in uric acid (+143.68 µmol/L difference) is a well-known fasting side effect, caused by reduced renal excretion and accelerated purine turnover during ketosis. In individuals prone to gout, this warrants attention. 1
The figure makes the rebound visible
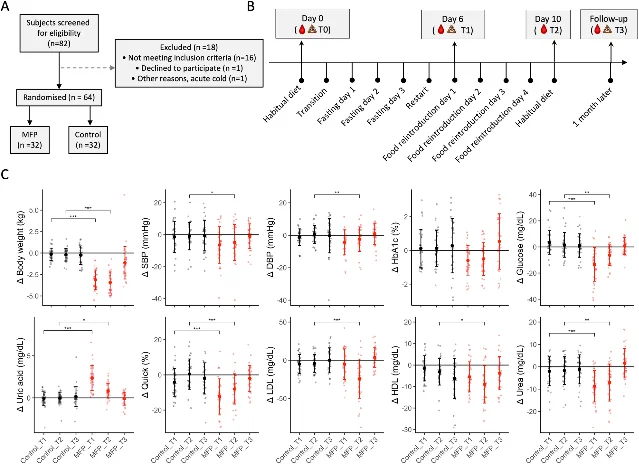
The scatter plots in panel C tell the central story at a glance. In the MFP group (red), body weight, glucose, LDL, and urea all show clear T1/T2 separation from controls — but by T3 (one month later) each trajectory converges back to the control band. The serum metabolomics data reinforces this: 24 metabolites fell and 9 rose during the fast, including a strong rise in ketone bodies (acetoacetate and 3-hydroxybutyrate), with amino acid concentrations dropping across the board. The chronic inflammation marker GlycA (a glycoprotein acetylation signal in NMR spectroscopy that tracks systemic inflammation) also declined. All of these returned to baseline at the one-month follow-up. 1
Who benefits more
The trial ran in healthy adults, but pre-specified subgroup analyses suggest higher-risk individuals saw larger effects:
- BMI > 25: greater BMI reduction (p = 0.006)
- Baseline total cholesterol > 200 mg/dL: LDL dropped an additional 19.7 mg/dL (p = 0.02)
- LDL > 130 mg/dL at baseline: LDL fell 16.8 mg/dL more than controls (p = 0.02)
- Higher diastolic blood pressure: greater diastolic reduction at T2 (p = 0.009)
This pattern — larger absolute benefit in those starting further from optimal — mirrors what is seen in caloric restriction and fasting-mimicking diet (FMD) trials more broadly. 1
The gut microbiome data followed the same transient arc. Eleven bacterial species shifted significantly in relative abundance during the fast, and 52 carbohydrate-active enzyme (CAZyme — proteins that break down complex carbohydrates) families changed in a consistent direction — reduced fiber-degrading enzymes, increased host glycan-degrading enzymes — indicating the gut microbiome switches from dietary substrates to host-derived substrates when dietary fiber drops sharply. At one month, microbiome composition had fully reverted. 1
What peer review changed
This study went through an unusually visible revision process. The preprint posted on medRxiv in November 2024 3 made claims that the published Genome Medicine version, released in June 2026 after approximately 18 months of peer review, no longer supports:
Conclusion language: the preprint concluded the MFP "effectively improves cardiometabolic health and emotional well-being." The published version reads "transiently improves cardiometabolic health and physical well-being." Three changes compressed into that one sentence — "effectively" became "transiently," emotional well-being was removed entirely, and the framing shifted from promotion to restraint.
Blood pressure: the preprint reported a significant T1 drop in systolic BP (−6.4 ± 11.5 mmHg, p = 0.03) and diastolic BP (−4.4 ± 7.7 mmHg, p = 0.05). The published version applied Bonferroni correction to the primary endpoints, and those same results fell to p = 0.08 (SBP) and p = 0.13 (DBP) — no longer significant.
Statistical reporting: published results use linear mixed-model estimates ± SE rather than raw means ± SD, making the headline numbers harder to parse without reading the full tables. The preprint's "−3.1 kg weight loss" became "−0.55 ± 0.02 kg/day difference" in the published version — the same underlying finding, but expressed in a way that is less immediately intuitive.
These are normal outcomes of rigorous peer review, and they reflect well on Genome Medicine's process. But they are also a reminder that preprint figures circulated widely for over a year before the corrected version appeared. 1 3
Limitations
The authors identified four limitations. The sample is predominantly healthy, Caucasian adults; they explicitly note difficulty generalizing to patients with hypertension, type 2 diabetes, or fatty liver disease — exactly the populations most likely to try an at-home fasting kit. The intervention bundles multiple components (caloric restriction, ketogenic macronutrient ratio, ω-3-rich oils, mineral supplements, and educational materials), so no single element can be isolated as the active driver. Comfort and well-being outcomes were self-reported. And all metabolic and microbiome effects returned to baseline within one month; evidence on optimal repeat frequency and long-term effects is absent. 1
Funding and conflicts of interest are the most significant caveat in the study. First author Franziska Grundler, co-author and corresponding author Robin Mesnage, Alfred Holley, and Françoise Wilhelmi de Toledo are all employed by Buchinger Wilhelmi Development and Holding GmbH — the company that produces and sells the FASTING BOX evaluated in the trial. Three additional authors (Selina Strathmeyer, Steffen Heelemann, Roland Geyer) are employed by Lifespin GmbH, which provided the metabolomics analysis. The remaining five authors declared no conflicts. 1
This COI structure — manufacturer-employed researchers testing a proprietary product — does not automatically invalidate the results, and the RCT design with a concurrent control group provides a structural safeguard. However, readers and clinicians should weight independent replication accordingly.
On generalizability: n = 64 (32 per arm) is underpowered to detect effects in subgroups with specific metabolic conditions. The one-month follow-up is too short to assess whether repeated cycles produce durable change. The clinic recruitment setting (participants were screened at a fasting specialist clinic) may select for people already motivated to fast, limiting external validity.
The recommendation
For a health-conscious adult or dietitian evaluating whether a 5-day, 623 kcal/day plant-based fasting kit is worth doing, here is what the current evidence actually supports:
Based on this trial, a single 5-day cycle at 623 kcal/day will likely produce a drop of roughly 3 kg in body weight and approximately 17 mg/dL in fasting blood glucose, with LDL continuing to fall during the 4-day reintroduction phase. People starting with LDL above 130 mg/dL or BMI above 25 see larger absolute drops.
What this trial does not support: sustained blood pressure reduction from a single cycle, or any durable metabolic benefit extending beyond four to six weeks without repeating the protocol.
Several groups should not attempt this without medical supervision: individuals prone to gout (uric acid spikes sharply), those on anticoagulants (the published data show an INR increase of 0.06 and a PTT — a measure of blood clotting time — prolongation of 1.0 s), pregnant or breastfeeding women, and anyone with a history of disordered eating.
For a patient with mildly elevated LDL (130–159 mg/dL) or fasting glucose creeping toward pre-diabetic range, this trial provides plausible mechanistic support for a short fasting cycle — but the gains will likely revert within a month unless dietary habits change during and after reintroduction. The reintroduction phase appears to carry as much metabolic weight as the fast itself; a 4-day transition back to a high-fiber, lower-saturated-fat diet is not optional. The trial authors frame the kit as a "non-pharmacological strategy" that "empowers individuals to explore and manage their own dietary strategies" rather than a standalone therapy — that framing fits the evidence. 1
正在加载内容卡片…
正在加载内容卡片…
Cover image: AI-generated illustration.
围绕这条内容继续补充观点或上下文。