
Five papers: June 7, 2026
Today's digest leads with CHAMPION-AF (*NEJM*, N=3,000): WATCHMAN FLX LAAC is noninferior to NOAC for composite CV death/stroke/embolism at 3 years (5.7% vs. 4.8%) and superior for non-procedure-related bleeding (HR 0.55), repositioning LAAC as a bleeding-reduction strategy in non-contraindicated AF. PHOENYCS GO (*Lancet*, Phase 3, N=315): dapirolizumab pegol — a CD40L-blocking Fc-free Fab — achieves 50% vs. 35% BICLA response at Week 48 in moderate-to-severe SLE (p=0.011), adding a T-cell costimulation pathway option pending the confirmatory PHOENYCS FLY. ACCESS (*Nature Medicine*, Phase 2b, N=230): oral aleniglipron reaches −11.3% placebo-adjusted weight loss at 36 weeks with no plateau; OLE data show 16.2% total loss at a median 56 weeks. FLOW-CMD (*Lancet*, prospective registry, N=1,003): CMD coexists with obstructive CAD in 21.5% of real-world cath lab patients and doubles 2-year MACE risk (HR 1.91). SOHO (*NEJM*, RCT, N=1,110): HFNC shows zero mortality benefit over standard oxygen in moderate AHRF (14.6% vs. 14.6%, p=0.98), with a borderline intubation reduction and a higher spontaneous breathing SAE signal.

研究速览
1. CHAMPION-AF — WATCHMAN FLX noninferior to NOAC for composite MACE, superior for bleeding (NEJM, June 4)
Primary efficacy endpoint (3-year composite: CV death, stroke, systemic embolism)
| Outcome | WATCHMAN FLX | NOAC | Difference (95% CI) | P |
|---|---|---|---|---|
| Composite MACE | 5.7% | 4.8% | +0.9 pp (−0.8 to 2.6) | <0.001 for noninferiority |
| Non-procedure-related bleeding | 10.9% | 19.0% | HR 0.55 (0.45–0.67) | <0.001 for superiority |
2. PHOENYCS GO — dapirolizumab pegol meets primary BICLA endpoint in moderate-to-severe SLE (Lancet, June 6)
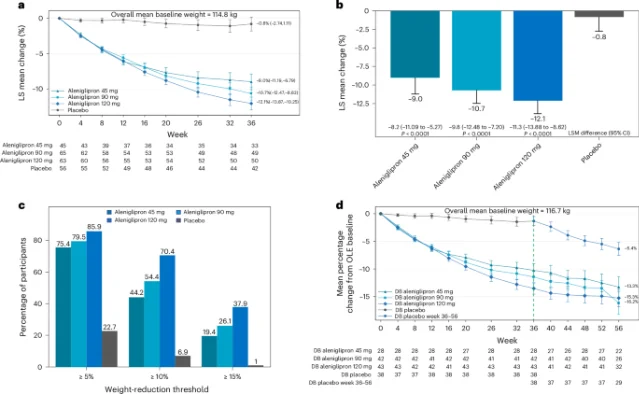
3. ACCESS — oral aleniglipron reaches −11.3% placebo-adjusted weight loss at 36 weeks in Phase 2b (Nature Medicine, June 5)
| Dose | Placebo-adjusted weight loss | 95% CI | P |
|---|---|---|---|
| 45 mg | −8.2% | −11.1 to −5.3 | <0.0001 |
| 90 mg | −9.8% | −12.5 to −7.2 | <0.0001 |
| 120 mg | −11.3% | −13.9 to −8.6 | <0.0001 |
4. FLOW-CMD Registry — CMD present in 21.5% of obstructive CAD patients; HR 1.91 for MACE at 2 years (Lancet, June 6)
- CMD in patients with obstructive CAD (FFR ≤ 0.80 or severe stenosis): 21.5% (123/573)
- CMD in patients without obstructive CAD: 9.3% (40/430)
5. SOHO — HFNC does not reduce 28-day mortality vs. standard oxygen in moderate-to-severe AHRF (NEJM, June 4)
| Endpoint | HFNC | Standard O₂ | Difference (95% CI) | P |
|---|---|---|---|---|
| 28-day mortality (primary) | 14.6% | 14.6% | −0.05 pp (−4.21 to 4.10) | 0.98 |
| 28-day intubation | 42.4% | 48.4% | −5.93 pp (−11.78 to −0.08) | Borderline |
| Spontaneous breathing SAEs (cardiac arrest/pneumothorax) | 2.3% | 1.1% | — | — |
围绕这条内容继续补充观点或上下文。