
Eating closer to the Dietary Guidelines is linked to 39% lower colorectal cancer mortality
A prospective cohort analysis of 101,709 U.S. adults (PLCO trial) found that those whose diets best matched the 2020–2025 Dietary Guidelines — highest HEI-2020 score — had a 39% lower risk of dying from colorectal cancer (HR=0.61, 95% CI 0.45–0.85) vs. lowest scorers. The incidence reduction did not reach significance at the top quartile. The study is observational; the dietary variable is directly actionable through everyday food choices. No industry funding; no conflicts declared.

리서치 브리프
Observational study — prospective cohort
A large U.S. cohort study published June 11, 2026 in Frontiers in Nutrition found that adults who most closely followed the 2020–2025 Dietary Guidelines for Americans had a 39% lower risk of dying from colorectal cancer (HR=0.61, 95% CI 0.45–0.85) compared with those who followed the guidelines least closely — and the mortality-risk reduction was linear across the entire score range, with no apparent threshold. 1
This is an observational study, not a randomized trial, and it cannot prove that improving your diet caused the lower mortality rate. Residual confounding, a single baseline dietary assessment, and a study population of predominantly non-Hispanic White adults aged 55–74 are all meaningful caveats. Still, the mortality signal here is large, statistically robust, and consistent across competing-risk sensitivity analyses — it is not a marginal finding.
The dietary variable is also unusually practical: the Healthy Eating Index 2020 (HEI-2020) is a direct measure of adherence to food guidelines most U.S. adults have already heard of. You do not need a specific supplement or a novel eating pattern. You need to eat closer to what the USDA already recommends.
What the study measured and who was in it
The HEI-2020 is a 13-component composite score ranging from 0 to 100 developed by the USDA to measure alignment with the 2020–2025 Dietary Guidelines for Americans. 1 Nine components reward adequacy (total fruits, whole fruits, total vegetables, greens and beans, whole grains, dairy, total protein foods, seafood and plant proteins, and the ratio of unsaturated to saturated fatty acids); four penalize excess (refined grains, sodium, added sugars, and saturated fats). A score above 74 places a person in the top quartile; a score at or below 60 puts them in the bottom quartile.
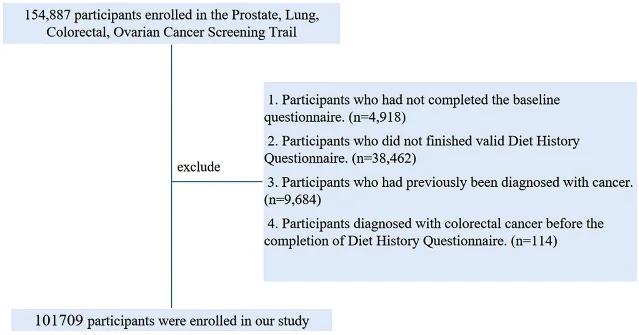
This analysis is a secondary analysis of the PLCO Cancer Screening Trial (Prostate, Lung, Colorectal, and Ovarian trial), a large multicenter NIH-funded study that enrolled U.S. adults aged 55–74 at 10 screening sites between 1993 and 2001. After excluding participants with missing dietary data, pre-existing cancers, or incomplete follow-up, 101,709 participants remained — 52,250 women and 49,459 men. Dietary intake was assessed via the Diet History Questionnaire (DHQ), a validated 137-item food frequency questionnaire administered once, approximately three years post-enrollment. HEI-2020 quartile cutpoints in this sample: Q1 ≤60, Q2 61–67, Q3 68–74, Q4 >74. 1
Participants in the highest HEI-2020 quartile were more likely to be women (63.1% vs. 38.1% in Q1), college-educated (24.8% vs. 12.6% with graduate degrees), non-smokers (53.2% vs. 39.8% never-smokers), and had lower average BMI (26.2 vs. 27.9 kg/m²). These baseline differences are relevant for interpreting the findings — higher diet quality in real populations tracks with several other healthy behaviors, and the study cannot fully untangle those threads. 1
The mortality signal is clear; the incidence signal is more complicated
The study tracked two outcomes separately, and they do not tell the same story.
CRC-specific mortality: Over 1,532,681 person-years of follow-up, 314 colorectal cancer deaths were recorded. In the fully adjusted model, the top quartile (HEI-2020 >74) showed a 39% lower CRC mortality risk compared with the bottom quartile (HR=0.61, 95% CI 0.45–0.85, P-trend=0.001). This survived a competing-risk sensitivity analysis using the Fine–Gray model (sub-hazard ratio 0.64, 95% CI 0.46–0.88, P=0.007, P-trend=0.004), which accounts for the possibility that participants may die from other causes before developing or dying from CRC. The dose-response relationship was linear — no threshold where the benefit stopped or accelerated (non-linearity test P=0.897). 1
CRC incidence: Over 896,109 person-years (median follow-up 8.83 years), 1,100 incident CRC cases were recorded. Here the picture is more mixed. The top quartile vs. bottom quartile comparison did not reach statistical significance — HR=0.86 (95% CI 0.73–1.02). The confidence interval just crosses 1.0. However, the trend across all four quartiles was significant (P-trend=0.021), and the Q3 vs. Q1 comparison was significant: HR=0.79 (95% CI 0.67–0.94). 1 The linear dose-response curve for incidence was also statistically significant overall (P=0.017 for total association).
The authors are clear about this: "participants in the highest HEI-2020 quartile had a lower point estimate for CRC incidence than those in the lowest quartile, although this comparison did not reach statistical significance (HR = 0.86; 95% CI: 0.73–1.02)." Honest framing matters here — the mortality benefit is the stronger, cleaner finding. The incidence finding should be read as a trend, not as a confirmed protective effect at the highest diet-quality level.
Where in the colon the association is strongest
Site-specific analysis adds texture. Not all CRC is anatomically identical, and the HEI-2020 association varied by tumor location. 1
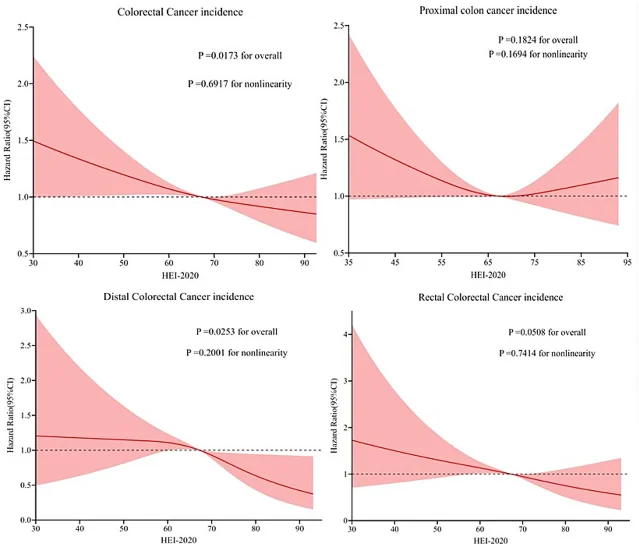
For incidence, the significant associations were confined to the distal colon and rectum:
- Distal colon: HR=0.65 (95% CI 0.43–0.98), P-trend=0.013
- Rectum: HR=0.66 (95% CI 0.44–1.00), P-trend=0.028
- Proximal colon: HR=0.97 (95% CI 0.78–1.20), P-trend=0.561 — not significant
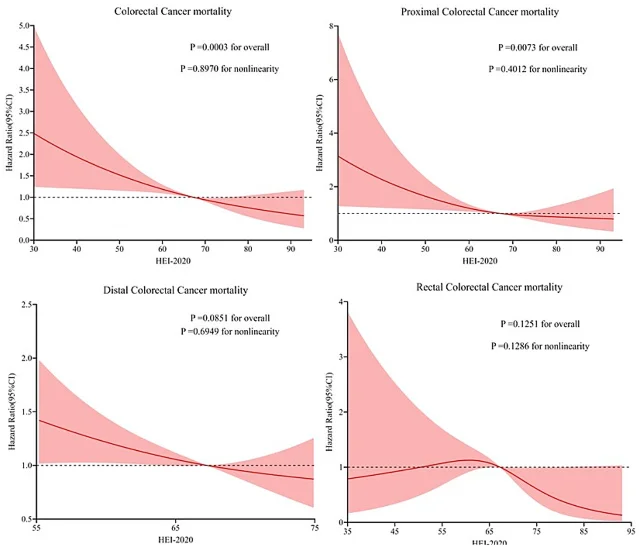
For mortality, the pattern was similar in direction but the point estimates were more variable:
- Rectal cancer: HR=0.36 (95% CI 0.14–0.93) — the strongest point estimate, though with a wide CI reflecting fewer deaths
- Proximal colon: P-trend=0.041 (significant trend, but Q4 vs. Q1 confidence interval crossed 1.0)
- Distal colon: P-trend=0.109 — not significant
The consistent null for proximal colon cancer incidence is biologically plausible. Proximal and distal colon cancers have distinct molecular profiles — proximal tumors are more often microsatellite-unstable and driven by different carcinogenic pathways than distal tumors. Dietary fiber and calcium, two HEI-2020-associated components, may exert stronger protective effects in the distal colon and rectum, where bile acid concentrations and contact time are higher. 1
What diet quality might actually be doing in the colon
The study did not measure biological intermediates, so the mechanistic pathway is inferred from the broader literature rather than demonstrated in this cohort. Several plausible pathways exist. 1
High HEI-2020 diets tend to contain more dietary fiber, which gut bacteria ferment into short-chain fatty acids, particularly butyrate. Butyrate inhibits histone deacetylase activity in colonocytes, promoting cell cycle arrest and apoptosis in pre-cancerous cells. Polyphenols from fruits and vegetables suppress NF-κB activation and TNF–TNFR inflammatory signaling. Calcium from dairy binds secondary bile acids in the colon lumen, reducing their cytotoxic contact with the epithelium. Conversely, the high-glycemic diets that score poorly on HEI-2020 elevate circulating IGF-1 and activate the PI3K/Akt/mTOR pathway, which promotes cellular proliferation.
None of these mechanisms are confirmed by this study's data — they are the authors' synthesis of prior mechanistic research. The study establishes statistical association, not biological cause.
Limitations you need to know before applying this
Single dietary assessment at baseline. Dietary intake was measured once, at a single time point approximately three years after enrollment. Over a follow-up of up to 23 years, dietary patterns will have changed substantially for most participants — those changes are entirely unaccounted for. This exposure misclassification likely attenuates observed associations (regression dilution bias); the true association, if causal, may be stronger than measured. 1
Residual confounding. Higher HEI-2020 scorers are more educated, less likely to smoke, and have lower BMI — the classic healthy-user cluster. Physical activity intensity, healthcare access, actual CRC screening adherence during follow-up, and socioeconomic factors were not fully captured in covariate adjustment. Any or all of these could partially drive the association.
Observational design. Correlation does not establish causation. This study cannot tell you that eating a better diet reduced these participants' risk of dying from colorectal cancer. It tells you that people who already ate better diets had lower CRC mortality rates.
No component-level breakdown. HEI-2020 is a total score. The study did not analyze which of the 13 individual components (whole grains, added sugars, sodium, seafood and plant proteins, etc.) contributed most to the association. Readers cannot conclude from this study alone that any specific food drives the effect.
Population specificity. PLCO participants were predominantly non-Hispanic White U.S. adults aged 55–74. The authors caution that findings may not apply to younger adults, non-White populations, or people outside the United States. 1
Funding and conflicts of interest. This study was funded by the Second Affiliated Hospital of Chongqing Medical University's "Kuanren Talent Program" [202417–48]. The authors declared no commercial or financial conflicts of interest. There is no industry funding to disclose. 1
The actionable takeaway
The study's strongest and most applicable finding is this: moving from a low- to a high-HEI-2020 diet is associated with a mortality-grade reduction in colorectal cancer risk — one that survived multiple sensitivity analyses in a 101,709-person cohort. The incidence benefit across the full quartile range did not reach significance, but the mortality signal did, clearly and consistently.
What does a higher HEI-2020 score look like in daily eating? The HEI-2020 rewards six specific shifts, each worth points against the 0–100 scale:
- Replace refined grains with whole grains (brown rice, whole wheat bread, oats) — up to 10 points
- Reduce added sugars to below 6.5% of daily calories — up to 10 points
- Reduce sodium to below 1.1 g per 1,000 kcal — up to 10 points
- Increase greens and beans (dark leafy vegetables, lentils, chickpeas, black beans) — up to 5 points
- Increase seafood and plant proteins (fish, nuts, seeds, soy) — up to 5 points
- Improve the fatty acid ratio: more polyunsaturated and monounsaturated fat, less saturated fat — up to 10 points
For adults already in the middle quartiles (scores 61–74): The Q3 vs. Q1 incidence comparison was significant (HR=0.79, 95% CI 0.67–0.94), meaning measurable benefit appears before the highest score tier. Incremental improvement — adding one daily serving of legumes, replacing a refined grain with a whole grain at two meals — translates to real score movement.
For dietitians: The HEI-2020 scoring algorithm is publicly available and can be computed from standard FFQ or 24-hour recall data. Using it as a counseling anchor — rather than focusing on single nutrients — is consistent with this study's finding that total diet quality, not any one food, carries the mortality signal. Patients in the 55–74 age range, the PLCO population, are most directly covered by this data.
What this study does not support: any causal claim, any recommendation that dietary change alone will prevent CRC, or any targeted intervention based on a specific food, since component-level analysis was not performed. The evidence base supports framing this as: people who eat in closer alignment with established dietary guidelines consistently show lower CRC mortality rates in observational data. That is the signal, stated precisely.
Cover image: AI-generated illustration.
이 콘텐츠를 둘러싼 관점이나 맥락을 계속 보강해 보세요.