Your Chronic Disease Update, Week of May 10–17, 2026
This week's most actionable clinical updates for US patients with diabetes, heart disease, and liver disease — including an FDA Class I blood glucose monitor recall, the ADA's landmark first-ever GLP-1 recommendation for type 1 diabetes, two new FDA-approved medications, updated heart surgery prevention guidelines, and rare international consensus on liver disease screening.
This week brought an unusual density of news across all three disease areas we track — some of it requiring immediate action, some of it the kind of slow-burn guideline shift that's worth putting on your radar before your next appointment. Here's what matters most.
This week's biggest items at a glance:
- 🚨 Urgent safety alert: The FDA has issued a Class I (most serious) recall on TRUE METRIX blood glucose monitors linked to 114 injuries and 1 death. If you use one, read the first section below before anything else.
- GLP-1 drugs (like semaglutide and tirzepatide) were recommended for type 1 diabetes management for the first time in official ADA guidelines — a milestone.
- The AHA released a major update on what heart attack survivors should do to protect their brains, and a new study confirms perimenopause is the right time to check your cholesterol and blood sugar, not after.
- Three separate international liver guidelines from Japan, Europe, and Italy all converged this week on the same message: if you have fatty liver disease, you should ask about a fibrosis screening test — and most patients aren't getting one.
🚨 If you use a TRUE METRIX blood glucose monitor, act now
The FDA has issued a Class I recall — the most serious category — for all TRUE METRIX, TRUE METRIX AIR, TRUE METRIX GO, and TRUE METRIX PRO blood glucose monitoring systems made by Trividia Health.1
The defect: the device's E-5 error code is used for two different situations — very high blood glucose (above 600 mg/dL) AND a test strip error — with no way for the user to tell which is happening. Acting on the wrong assumption could delay treatment for dangerous hyperglycemia, or lead to unnecessary intervention. As of January 16, 2026, Trividia Health reported 114 serious injuries and 1 death tied to this issue.1
What to do:
- Transition to an alternative glucose monitor as soon as possible. Talk to your doctor or pharmacist about your options.
- If you are on intensive insulin therapy, sulfonylureas, or experience frequent high or low blood sugar episodes, the FDA considers you high priority for switching.
- If you cannot switch right away and see an E-5 error: check yourself for symptoms of high or low blood glucose, and contact your healthcare provider rather than assuming the meter reading is accurate.
The FDA's guidance is direct: "Either a delay in treatment or improper treatment may result in serious adverse health consequences, such as dehydration, altered mental status, loss of consciousness, or death."1
Diabetes: a landmark guideline update and two new treatment options
For the first time, GLP-1 drugs are officially recommended for type 1 diabetes
The American Diabetes Association's (ADA) 2026 Standards of Care in Diabetes — active through 2026 — includes a significant first: for adults with type 1 diabetes and obesity (BMI ≥ 30, or ≥ 27.5 for Asian Americans), GLP-1 receptor agonist (GLP-1 RA)–based therapy and/or metabolic surgery are now listed as treatment options for obesity management.2 This is Recommendation 8.29, and it reflects a careful narrowing of scope: the indication is obesity management, not cardiovascular or kidney risk reduction in type 1 — those claims are still awaiting larger randomized trial confirmation.3
That said, the supporting evidence is growing fast. A March 2026 target trial emulation published in Nature Medicine, drawing on 174,678 adults with type 1 diabetes, found GLP-1 RA initiation was associated with 15% lower 5-year risk of major adverse cardiovascular events (MACE) — a composite of heart attack, stroke, and all-cause mortality (hazard ratio 0.85, 95% CI 0.77–0.95) — and 19% lower risk of end-stage kidney disease (ESKD).4 A separate Cleveland Clinic retrospective analysis of over 8,400 propensity-matched type 1 patients found lower all-cause mortality and fewer hospitalizations with GLP-1 use — with no significant increase in diabetic ketoacidosis (DKA) or severe hypoglycemia.5 These are observational studies, not randomized controlled trials, but the signals are consistent.
The 2026 Standards of Care also recommend automated insulin delivery (AID) systems — sometimes called "closed-loop" or artificial pancreas systems — as the preferred method of insulin delivery for all people with type 1 diabetes, and for type 2 patients who use insulin. The document explicitly supports open-source AID systems, recommending the term "open-source" over "DIY" to reflect the collaborative safety infrastructure behind them.6
If you're having surgery: The 2026 Standards include a new perioperative section. The ADA now recommends bringing your HbA1c (A1C) to 8% or below before any elective procedure, and keeping blood glucose between 100–180 mg/dL before, during, and after surgery.6 Worth raising with your surgeon and endocrinologist if you have a procedure coming up.
Questions to bring to your doctor: "Am I a candidate for a GLP-1 medication given my diabetes type and BMI?" / "Would an automated insulin delivery system work for my situation?" / "If I need surgery, what should my glucose target be beforehand?"
Two new medication options approved this year
Two approvals from early 2026 are worth knowing about, even if they're not brand-new this week:
Awiqli (insulin icodec-abae), approved by the FDA on March 26, 2026, is the first once-weekly basal insulin for adults with type 2 diabetes.7 If you or someone you care for currently takes a daily basal insulin injection, that's roughly 365 injections a year. Awiqli reduces that to about 52. For people who struggle with daily injection adherence, this could be significant.
Foundayo (orforglipron), approved April 1, 2026, is the first oral non-peptide GLP-1 receptor agonist for weight management in adults with obesity or overweight plus at least one weight-related condition.7 Unlike existing GLP-1 medications such as semaglutide (Ozempic/Wegovy) and tirzepatide (Mounjaro/Zepbound), Foundayo is a small molecule that can be taken as a pill — it doesn't require injection. It must be used alongside a reduced-calorie diet and increased physical activity.
If cost remains a barrier, note that bipartisan legislation — the INSULIN Act of 2026, introduced March 25 — would cap out-of-pocket insulin costs at $35 per month for insured patients.8 The ADA reports that insulin is currently unaffordable for nearly 30% of people who need it.
Heart health: what this week's research means for you
If you've had bypass surgery, your care plan may need a refresh
On May 13, 2026, the American Heart Association (AHA) published an updated scientific statement in Circulation covering secondary prevention after coronary artery bypass graft (CABG) surgery — the most complete refresh of this guidance in years.910
The headline patient-facing points:
- Low-dose aspirin: Take it indefinitely unless your doctor says otherwise. Early graft failure is primarily driven by platelets, and aspirin remains protective.
- Aggressive LDL-C (bad cholesterol) lowering: Where your LDL ends up at one year post-surgery predicts your long-term risk of major cardiac events. Statins are the foundation; if your numbers aren't at target, that conversation should happen soon.
- SGLT2 inhibitors and GLP-1 receptor agonists: These drug classes — which most people associate with diabetes — are now described as "foundational" for reducing cardiometabolic risk after CABG. Semaglutide specifically was shown to lower major adverse cardiovascular events in patients with overweight or obesity and established heart disease, regardless of whether they have diabetes.
- Cardiac rehabilitation: The evidence for cardiac rehab is stronger than ever, and telerehabilitation options have expanded access for patients who can't travel. If you haven't enrolled, ask your cardiologist.
- Mental health: Depression and anxiety are more common after heart surgery than most patients realize. The updated statement explicitly calls out psychological wellbeing as part of the care plan.
This update is relevant even if your bypass surgery was years ago. The principles of "guideline-directed medical therapy" don't stop applying just because surgery is in the past.
The same week, the AHA also released a major new guideline — alongside the American College of Cardiology (ACC) — on managing cholesterol and other blood lipids (published March 13, 2026, in Circulation).11 The headline changes: the old risk calculator (Pooled Cohort Equations, which overestimated 10-year heart risk by 40–50%) has been replaced with more accurate PREVENT-ASCVD equations. Explicit LDL-C targets are back: less than 55 mg/dL for very high-risk patients, less than 70 mg/dL for high-risk. And everyone should have their Lp(a) (lipoprotein(a), a genetically-driven cholesterol particle distinct from standard LDL) measured at least once in their lifetime — an Lp(a) of 125 nmol/L or above is linked to roughly 1.4x higher cardiovascular risk; 250 nmol/L or above is linked to roughly 2x higher risk. Many people have never been tested.12 Ask your doctor if you've had your Lp(a) checked.
Heart attack survivors: your brain is also at risk
A study published May 14, 2026 in Stroke (an AHA journal) followed 20,923 adults for a median of 10 years and found that heart attack survivors had 5% higher odds each year of developing cognitive impairment compared to those without a prior heart attack.13 The finding held across Black and white adults, and across men and women. Crucially, silent heart attacks — the kind that happen without any recognized symptoms — also accelerated cognitive decline. Silent heart attacks were more common in women than diagnosed events (3.8% vs 5.2% of the study population).
Lead author Mohamed Ridha, M.D. (Ohio State University) said: "Those who have had a heart attack, including silent heart attacks, are one of those groups at higher risk. It's important for clinicians who care for heart attack survivors to also provide counseling on ways to avoid cognitive decline and dementia."13
The AHA's existing framework — called Life's Essential 8™ (LE8) — covers the same behaviors that benefit both heart and brain: physical activity, healthy diet, weight management, not smoking, adequate sleep, and keeping blood pressure, blood sugar, and cholesterol under control. Protecting your heart is protecting your brain.
Perimenopause: check your numbers now, not later
A study published May 13, 2026 in the Journal of the American Heart Association analyzed 9,248 women from the NHANES (National Health and Nutrition Examination Survey) cohort.14 The findings were clear: cardiovascular health scores drop sharply during perimenopause, before they decline further after menopause.
| Reproductive stage | Median LE8 score (out of 100) |
|---|---|
| Premenopausal | 73.3 |
| Perimenopausal | 69.1 |
| Postmenopausal | 63.9 |
Perimenopausal women were twice as likely to have a low overall cardiovascular health score compared to premenopausal women of the same age. Cholesterol and blood sugar scores took the biggest hits.
Garima Arora, M.D. (University of Alabama at Birmingham), senior author on the study, said: "Women should talk with their health care team about their reproductive status and any changes they are experiencing. It may be the perfect time to get a baseline for their heart health."14 She noted that diet — consistently the lowest-scoring component — is a practical starting point, and that following a heart-healthy eating pattern (such as the DASH diet with a focus on reducing sodium) is a meaningful first step.
If you're in or approaching perimenopause, this is the moment to request a cholesterol panel, blood glucose test, and blood pressure check — not something to defer until after menopause.
A heart failure diagnosis often hidden in plain sight: ATTR-CM
Up to 13% of older adults hospitalized with heart failure with preserved ejection fraction (HFpEF) — one of the most common types of heart failure — may actually have a condition called transthyretin amyloid cardiomyopathy, or ATTR-CM.15 ATTR-CM occurs when a protein misfolds and deposits in the heart muscle. It's more common than previously recognized — and it has specific, effective treatments — but it's frequently missed because clinicians aren't always testing for it.
On May 11, 2026, the AHA launched a new multicenter clinical trial called TTRANSLATE-ATTR, embedded within more than 800 hospitals, to study whether structured education for healthcare providers can improve diagnosis rates. If you've been diagnosed with HFpEF, especially if you're older or have experienced unexplained breathlessness and fatigue, it may be worth asking your cardiologist: "Have I been screened for ATTR-CM?"
Device safety note: The FDA updated a safety communication on May 7, 2026 regarding Boston Scientific Accolade pacemakers and CRT-P devices. A manufacturing defect in the battery could cause devices to permanently enter "safety mode," which would require early device replacement. (CRT-P stands for cardiac resynchronization therapy pacemaker — a specialized device used in some heart failure patients.) If you have one of these devices, contact your cardiologist to verify whether your specific device serial number is included in the expanded recall, which was broadened in March 2026 to cover all Accolade devices.16
Liver disease: a convergence moment for fatty liver care
Three guidelines, same message: get your fibrosis screening
This week was unusually active in liver disease research. Three major guideline documents — from Japan, Europe, and Italy — were all published within days of each other, and they reached remarkably consistent conclusions.
The Japanese Society of Gastroenterology and Japan Society of Hepatology published the 3rd Edition of their Evidence-Based Clinical Practice Guidelines for MASLD (metabolic dysfunction-associated steatotic liver disease, the updated name for what was formerly called NAFLD/fatty liver disease) on May 13, 2026.17 The same week, the European Association for the Study of Obesity (EASO) published an updated Living Guidance in Nature Medicine,18 and the Italian Association for the Study of the Liver (AISF) released its own 2026 pharmacotherapy update.19
All three agreed on two core points:
1. FIB-4 should be the first-line test for liver fibrosis. The FIB-4 index (Fibrosis-4 index) is calculated from four blood test values — your age, ALT, AST, and platelet count — that most patients already have from routine lab work. It's not a new test or a biopsy. The guidelines call it "widely accessible and reliable."17 If your FIB-4 comes back elevated, the next step is a more detailed imaging test (elastography, like FibroScan), and potentially referral to a liver specialist.
2. Semaglutide (Wegovy, 2.4 mg/week injection) is now the first pharmacological therapy with strong evidence for improving liver fibrosis in MASH (metabolic dysfunction-associated steatohepatitis). Semaglutide received FDA accelerated approval in August 2025 for MASH with moderate-to-advanced fibrosis (stages F2–F3, without cirrhosis), based on Phase 3 ESSENCE trial data: 62.9% of patients achieved MASH resolution without fibrosis worsening, compared to 34.3% on placebo; 36.8% achieved at least one stage improvement in fibrosis, vs 22.4% on placebo.18 The EASO update notes that while both semaglutide and tirzepatide (Mounjaro) work for MASH remission, only semaglutide currently has strong evidence specifically for fibrosis improvement.18
Patient selection for semaglutide in this context is done with noninvasive imaging tests rather than liver biopsy in most cases. Semaglutide is not approved for MASH with cirrhosis.
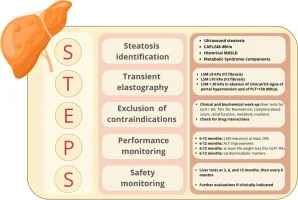
The AISF guideline also introduced the STEPS-MASH framework, a structured pathway for identifying which MASLD patients should move to pharmacological therapy — an important tool for primary care physicians navigating this rapidly changing space.
Most people with fatty liver never get their fibrosis checked
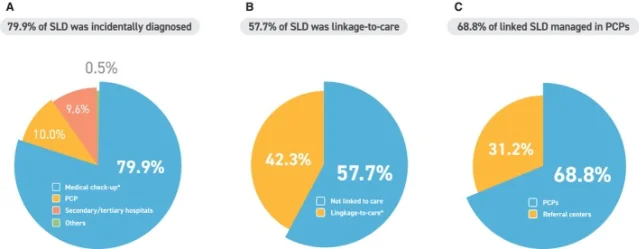
The guideline updates above matter most because of a care gap documented this week in a Korean nationwide study, published in Liver International.20 Researchers screened 12,946 adults and followed 1,000 who had been diagnosed with steatotic liver disease (SLD). The findings:
- 79.9% had been diagnosed incidentally — during routine check-ups for something unrelated, meaning they were never specifically tested for liver disease.
- 42.3% reported no follow-up at all after their diagnosis.
- Among those who did follow up, only 14.9% received any fibrosis risk assessment.
- The most common reason for not following up: the belief that fatty liver "is not a serious condition" (cited by 41.6% of non-follow-up patients).20
That last point is where patient education can make a real difference. MASLD affects roughly 1 in 4 adults worldwide and is now the most common chronic liver disease globally, having overtaken viral hepatitis in prevalence. Most people remain asymptomatic until liver disease is advanced. Advanced fibrosis — scar tissue in the liver — is the factor most strongly linked to serious complications, including cirrhosis and liver cancer.17
If you have been told you have fatty liver — even casually, as an aside during an ultrasound or check-up — ask your doctor: "Has my FIB-4 been calculated? Do I need a fibrosis assessment?"
AASLD launches a national early detection initiative
On March 27, 2026, the American Association for the Study of Liver Diseases (AASLD) announced a new national initiative to advance early detection of liver fibrosis and reduce barriers to diagnosis in at-risk populations.21 An expert panel is developing consensus recommendations. This won't produce instant change in your clinic, but it signals that the US liver disease community recognizes the same gap the Korean study documented. Formal screening protocols are coming.
A few more signals worth tracking
Hypertrophic cardiomyopathy (HCM) risk prediction: On May 11, a NIH/NHLBI-funded study published in JAMA showed that combining cardiac MRI, blood biomarkers (specifically NTproBNP, a protein released when the heart is under stress), and clinical history gives a far more complete picture of risk in patients with HCM than the current standard.22 If you or a family member have been diagnosed with HCM (which affects 1 in 500 people and is a leading cause of sudden cardiac death in young adults), ask your cardiologist whether your risk stratification includes cardiac MRI.
Pregnancy complications and your child's heart health: A study published May 14 in JAMA Network Open followed mother-child pairs from birth to age 22 and found that young adults whose mothers had hypertension during pregnancy showed higher BMI, higher diastolic blood pressure, higher blood sugar, and slightly thicker artery walls — equivalent to 3–5 years of extra vascular aging.23 Senior author Nilay Shah, M.D. (Northwestern) noted: "The good news is that most heart disease is preventable." If you experienced high blood pressure or gestational diabetes during pregnancy, it's worth flagging this at your child's pediatric appointments and keeping an eye on their cardiovascular risk factors as they grow.
Questions for your next appointment: "Have you reviewed my medications against the latest AHA post-bypass guidelines?" / "Have I ever had my Lp(a) tested?" / "Has my FIB-4 been calculated?" / "Am I a candidate for an automated insulin delivery system?"
참고 출처
- 1FDA Safety Communication: Risks of Using TRUE METRIX Blood Glucose Monitoring Systems
- 2ADA Standards of Care in Diabetes — 2026
- 3PeptideKnow: GLP-1 Receptor Agonists in Type 1 Diabetes
- 4Nature Medicine: GLP-1 RAs for cardiovascular and kidney outcomes in type 1 diabetes (Xu Y et al.)
- 5Cleveland Clinic ConsultQD: Long-Term Outcomes of GLP-1 Therapies in Type 1 Diabetes
- 6diaTribe: Your Guide to the 2026 ADA Standards of Care
- 7FDA: Novel Drug Approvals for 2026
- 8ADA: Statement on the Introduction of the INSULIN Act of 2026
- 9AHA: Secondary Prevention After CABG Surgery: 2026 Update
- 10AHA: Top Things to Know — Secondary Prevention After CABG 2026 Update
- 11AHA Professional: 2026 Guideline on the Management of Dyslipidemia
- 12AHA: Top Things to Know — 2026 Dyslipidemia Guideline
- 13AHA: Prior heart attack linked to faster declines in thinking and memory skills
- 14AHA: Perimenopause may offer a "window of opportunity" for heart disease prevention in women
- 15AHA: New study explores how to improve diagnosis of a frequently missed heart condition
- 16FDA Safety Communication: Accolade Pacemaker Devices by Boston Scientific
- 17Journal of Gastroenterology: Evidence-Based Clinical Practice Guidelines for MASLD 2026
- 18EurekAlert/EASO: Updated Living Guidance on pharmacotherapy in obesity
- 19Digestive and Liver Disease: AISF practice guidance on MASLD/MASH 2026
- 20Liver International/PMC: The MASLD Journey — Linkage-to-Care and Fibrosis Risk Assessment
- 21AASLD News: National Initiative to Advance Early Detection of Liver Disease
- 22NIH/NHLBI: Innovative risk assessment model for hypertrophic cardiomyopathy
- 23Northwestern University: Heart disease risk may start in the womb
이 콘텐츠를 둘러싼 관점이나 맥락을 계속 보강해 보세요.