
Measles is back in a big way — here's what you actually need to know
The US hit 2,000+ confirmed measles cases by June 2026 — the worst pace since the 1990s. Here's why people your age might not be as protected as they assume, what the disease actually feels like, and the quick steps to check your MMR status.

The US has already logged over 2,000 confirmed measles cases in 2026. It's only June. Last year was the worst in 34 years, and we're already on pace to blow past it.
This isn't a scare story about a disease that only hits babies. A meaningful slice of 2026 cases are people your age — and if you were born in the early-to-mid 2000s, there's a real chance your protection isn't as solid as you think.
Here's what's actually happening and what you should do about it.
The numbers are unusually bad
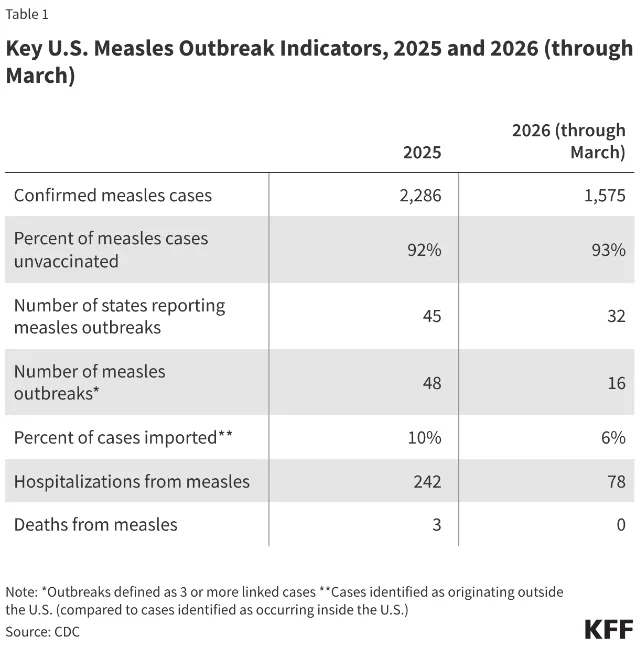
As of June 4, 2026, there are 2,030 confirmed measles cases across 40 US states and Washington DC — and 93% of them are linked to active outbreaks.1 For context: in all of 2024 there were only 285 cases. That's a roughly 7x jump in active outbreak pressure between 2024 and now.
차트를 불러오는 중…
South Carolina had the biggest single outbreak (669 cases), now over. Utah still has 486. Texas, Florida, and several other states have ongoing clusters.
72% of 2026 cases are in children and young adults up to 19 years old. Adults over 20 make up the remaining 27% — which is unusually high by historical measles standards.2 Six percent of patients have been hospitalized this year.
Why is it spreading so fast? A short, uncomfortable answer: vaccination rates have been falling for years. MMR coverage among kindergartners dropped from 95.2% in 2019-2020 to 92.5% in 2024-2025 — putting roughly 286,000 kindergartners at risk in the last school year alone.1 Below 95% coverage is where measles finds room to run.
Why Gen Z specifically should care
Most public health messaging around measles focuses on babies and unvaccinated kids, which makes sense — they're at highest clinical risk. But there's a specific vulnerability for people born in the late 1990s and early 2000s that doesn't get talked about much.
The MMR two-dose schedule wasn't standard until 1989. If you were born just before or around that window, your parents may have only gotten you one dose — which is 93% effective, not the 97% you get from two.3 That's a meaningful gap when measles is circulating in your state.
Beyond the schedule change, there's the pandemic disruption problem. COVID-19 caused widespread delays in routine childhood vaccines. A chunk of people who are now 18-21 may have gotten their second MMR dose late, missed a follow-up, or never had it documented properly.
And then there's the paperwork problem. A lot of people simply don't know their status because their childhood vaccine records have been lost, changed providers, or were never properly transferred. If you've ever moved, changed pediatricians, or aged out of your parents' health plan without thinking about this, your actual documented immunity may be a question mark.
The CDC specifically calls out students at post-high school educational institutions as a group that should make sure they have two documented MMR doses.3 College dorms and shared living situations are exactly the kind of close-contact environment where measles spreads efficiently.

What measles actually feels like
This matters because a lot of people in their 20s have never seen measles and don't know what to watch for.
It doesn't start with the rash. The first 4-5 days feel like a bad cold: high fever (can exceed 104°F), persistent cough, runny nose, red watery eyes.5 You might also notice tiny white spots inside your mouth — those are called Koplik's spots and they're almost diagnostic.
Then, 3-5 days into symptoms, the rash appears. It starts at the hairline and spreads downward across the body over a few days. By the time the rash shows up, you've probably been contagious for 4 days already — which is the part that makes measles so hard to contain.
The "it's just a rash" framing dramatically undersells the disease. About 30% of measles cases develop complications — ear infections, diarrhea, pneumonia, and in rare cases, brain inflammation.6 Around 1 in 1,000 infections lead to death. The hospitalization rate in 2025 was 11% — that's not trivial.
One thing that often surprises people: measles can linger in a room for up to two hours after an infected person has left. You don't need to be near them. You just need to breathe the same air they breathed.
The elimination status situation
In 2000, the US officially eliminated measles — meaning there was no longer any sustained domestic spread, only imported cases that occasionally sparked short chains. That was a major public health achievement held for 25 years.
That status is now seriously in jeopardy. In November 2025, the Pan American Health Organization placed the US in the category of "sustained with major concerns" — a step down from full elimination status.6 Technically losing elimination status requires 12 months of continuous domestic transmission — we're not there yet, but the pace of 2025-2026 outbreaks is pushing toward that line.
Why does it matter? Elimination status isn't just a trophy. It shapes how other countries view travel to the US, how healthcare providers triage fever cases in travelers, and how much ongoing monitoring and vaccination pressure public health agencies apply. Losing it would mean measles becomes an endemic concern requiring constant management rather than a rare import to extinguish.
What to actually do
This breaks down into two questions: do you have adequate protection, and what do you do if you think you've been exposed?
Figuring out your protection:
- Look up your vaccination records. Your state's immunization registry probably has them — most states have online portals. Your childhood pediatrician's office may also still have records.
- If you can find documentation of two MMR doses, you're almost certainly fine.
- If you have one documented dose, you're still 93% protected — but getting a second dose makes sense, especially if you live in a state with active outbreaks, travel internationally, or spend a lot of time in crowded environments.
- If you have no records or unknown status, just get two doses. It's safe to get MMR even if you're already immune — there's no harm in a redundant dose.3 Your campus health center, a pharmacy, or a Vaccines for Children-eligible clinic can do it.
If you think you've been exposed:
- Act fast. If you get an MMR vaccine within 72 hours of exposure, it may prevent infection or reduce severity.3
- If you're immunocompromised or can't get the vaccine for medical reasons, immune globulin given within 6 days can help.
- Don't go to a crowded urgent care if you think you have it — call first. Measles in a waiting room is how outbreaks spread.
- Watch for the symptom timeline: high fever + cough + runny nose + red eyes comes before the rash by several days. If you've had measles exposure and develop that cluster of symptoms, isolate immediately and call your healthcare provider.
The cost side:
Most health insurance covers MMR. If you don't have coverage, the Vaccines for Children program covers anyone 18 or younger, and many pharmacies and community health clinics offer low-cost adult vaccination.
The bigger context
The spike in measles cases isn't happening in a vacuum. Kindergarten MMR coverage has been falling for six straight years. Vaccine hesitancy increased after COVID. Federal funding for public health immunization programs has been cut. Some states have vaccination rates well below the 95% threshold — Idaho's was 78.5% in 2024-2025.6
A new Nature Health study mapping county-level MMR coverage found that in two states — New Mexico and Texas — parental-reported vaccination rates were dramatically lower than official estimates (61% vs. 90% in New Mexico, 63% vs. 94% in Texas), and those two states had the most significant measles outbreaks at the time of the analysis.7
The gap between official numbers and ground-level reality in some communities is probably bigger than the reported statistics suggest.
For you personally, this matters less as a political story and more as a practical one: measles is actually spreading in the US right now, it's spreading faster than it has in decades, and if your vaccine status is uncertain, checking it takes 20 minutes.
참고 출처
- 1CDC Measles Cases and Outbreaks — June 2026
- 2US measles cases top 2,000 in just 5 months — CIDRAP
- 3CDC Measles Vaccination — vaccine effectiveness data
- 4Photo by Gustavo Fring — Pexels
- 5CDC Measles Symptoms and Complications
- 6KFF — Measles Elimination Status: What It Is and How the U.S. Could Lose It
- 7CIDRAP — New US map of MMR vaccine uptake reveals considerable gaps
이 콘텐츠를 둘러싼 관점이나 맥락을 계속 보강해 보세요.