
Vegetarian diets did not reduce CRP in clinical trials — the inflammation benefit may take years, not weeks
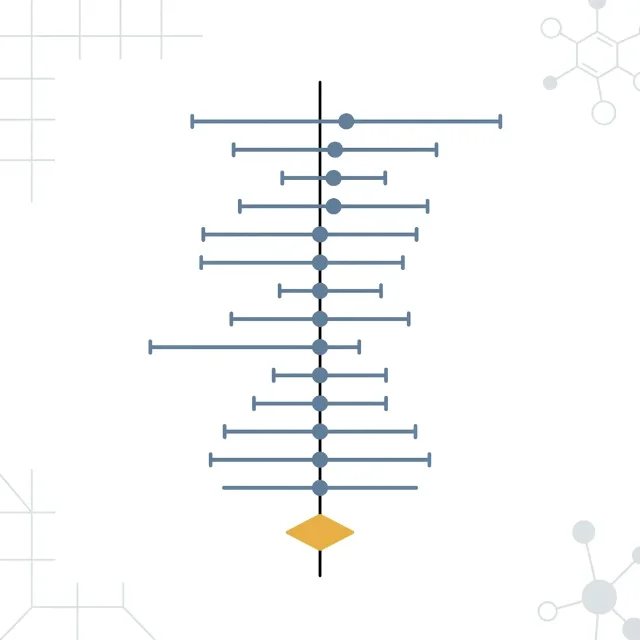
A meta-analysis of 10 RCTs (N=545, I²=0.0%) published June 9, 2026 in BMC Nutrition found that vegetarian diets produced no statistically significant change in C-reactive protein compared with omnivorous control diets (WMD −0.04 mg/L, 95% CI −0.23 to 0.15, p=0.683). All 12 subgroup analyses — by diet strictness, baseline CRP, duration, BMI, sex, age, and health status — were non-significant. GRADE certainty is moderate; no COI. The authors propose a time-lag hypothesis: the CRP benefit observed in long-term observational studies may not materialize within the weeks-to-months timescales that RCTs test. Actionable takeaway: CRP is not a reliable short-term biomarker of dietary progress for vegetarian diet switchers; dietitians seeking CRP reduction within weeks should prioritize weight loss, Mediterranean patterns, or UPF reduction instead.

リサーチノート
What the researchers measured and why CRP matters
The 10 trials: who was studied and for how long
| Parameter | Range |
|---|---|
| Total participants | 545 adults |
| Individual trial size | 23–100 participants |
| Countries | USA (6), Sweden (2), Czech Republic (1), Germany (1) |
| Vegetarian diet types | Vegan (7 arms), lacto-ovo-vegetarian (3), lacto-vegetarian (1) |
| Trial duration | 3 weeks to 74 weeks |
| Health conditions | Healthy adults (5 trials), T2DM (2), ischemic heart disease (1), coronary artery disease (1), rheumatoid arthritis (1) |
| Mean age range | 27–68 years |
The result: null across every subgroup
- By baseline CRP: Participants with elevated CRP (≥3 mg/L) showed a directionally larger effect (WMD −0.56 mg/L) but still not significant (p = 0.176). Participants with CRP below 3 mg/L: WMD −0.01 (p = 0.921).
- By diet type: Vegan arms (WMD −0.05, p = 0.719) and non-vegan vegetarian arms (WMD −0.28, p = 0.453) did not differ from each other (p-between = 0.568).
- By trial duration: Trials longer than 8 weeks (WMD −0.52, p = 0.364) showed no benefit over shorter trials (p-between = 0.395).
- By BMI, sex, age, health status: All non-significant in both directions.

Why the RCTs and the observational data disagree
Quality of evidence: what GRADE moderate means here
Where this sits in the existing evidence base
このコンテンツについて、さらに観点や背景を補足しましょう。