
Daily sauerkraut cuts systolic blood pressure ~2 mmHg — fresh or pasteurized, it doesn't matter
A 2026 randomized crossover trial (n=87 healthy adults, EJCN) finds 100g/day sauerkraut reduces SBP ~2 mmHg; pasteurized works as well as fresh; no CRP or glucose benefit in overall population.

リサーチノート
Randomized crossover trial | European Journal of Clinical Nutrition (Nature), published June 19, 2026 · DOI: 10.1038/s41430-026-01776-5 · Open access, CC BY 4.0
Fermented vegetables have accumulated a reputation — often loosely attributed to their probiotic content — for improving gut health, dampening inflammation, and supporting metabolic markers. A 2026 randomized crossover trial published in the European Journal of Clinical Nutrition puts that reputation to a controlled test, and the result is more precise, and considerably more modest, than the general enthusiasm suggests. 1
The bottom line: 100g of sauerkraut per day for four weeks reduced systolic blood pressure by roughly 2 mmHg in healthy adults. Both fresh (probiotic-active) and pasteurized (bacteria inactivated) sauerkraut produced identical reductions. For every other marker tracked — C-reactive protein, IL-6, fasting glucose, insulin, and three separate gut barrier integrity proteins — the overall population saw no statistically significant benefit.
Study design and who was enrolled
Researchers at the University of Freiburg, Germany recruited 87 healthy adults (84 completers) in a monocentric randomized crossover design between October 2021 and August 2022. 1 Each participant completed two four-week intervention phases — 100g/day of fresh sauerkraut and 100g/day of pasteurized sauerkraut — each preceded by a four-week washout period. The crossover design means every participant served as their own control, substantially increasing statistical power for within-person comparisons.
Participant demographics: mean age 44.4 ± 14.0 years (range 21–69), mean BMI 24.1 ± 3.0 kg/m² (range 18.1–30.8), 56.3% female (n = 49), 43.7% male (n = 38). Mean daily fiber intake at baseline was 23.8 ± 9.0 g/day. 2 The enrollment criteria excluded people with diabetes, hypertension, gastrointestinal disease, cardiovascular events, recent antibiotic use, veganism, and eating disorders — the study population was, by design, healthy.
The two intervention products were sourced from a single commercial brand (EDEN, Hügli Nahrungsmittel GmbH, Radolfzell, Germany). Fresh sauerkraut carried live Lacticaseibacillus paracasei at approximately 1.4–3.2 × 10⁵ CFU/mL — notably below the 1 × 10⁹ CFU/serving threshold typically cited as the minimum for a probiotic effect. Pasteurized sauerkraut was heat-treated at 75°C for five minutes, reducing CFU to below detection. Salt content differed slightly: 0.8% in fresh sauerkraut versus 1.2% in pasteurized, adding about 0.4g of extra sodium per day in the pasteurized arm. 1
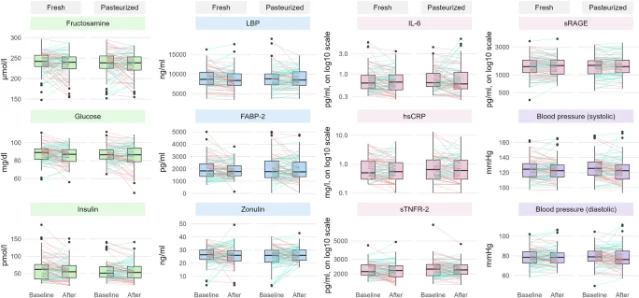
Twelve outcomes were tracked across four categories: blood pressure (systolic and diastolic), inflammatory markers (hsCRP, IL-6, sTNFR-2, sRAGE), metabolic markers (fasting glucose, fructosamine, fasting insulin), and gut barrier integrity markers (LBP, FABP-2, zonulin). Statistical modeling was outcome-specific — Gamma regression for log-normally distributed markers, normal linear regression for the rest — with 83.8% explained deviance for the blood pressure model. 3
What changed — and what didn't
The table below summarizes the primary outcomes from the regression models. 3
| Outcome | Baseline | Fresh sauerkraut | Pasteurized sauerkraut | Significant? |
|---|---|---|---|---|
| Systolic BP | 132.2 mmHg | −1.6% (95% CI −3.0% to −0.2%), p = 0.022 | −1.5% (95% CI −2.8% to +0.1%), p = 0.040 | ✅ Both |
| Diastolic BP | 83.2 mmHg | +0.3% (p = 0.696) | −1.2% (p = 0.141) | ❌ Neither |
| hsCRP | 0.91 mg/L | −13.2% (95% CI −25.8% to +1.4%), p = 0.076 | −9.0% (p = 0.236) | ❌ Neither |
| IL-6 | 0.87 pg/mL | −9.7% (p = 0.106) | +2.2% (p = 0.727) | ❌ Neither |
| sTNFR-2 | 2,325 pg/mL | −2.9% (p = 0.087) | −1.1% (p = 0.537) | ❌ Neither |
| Fasting glucose | 91 mg/dL | −1.8 mg/dL (p = 0.115) | −2.2 mg/dL (p = 0.053) | ❌ Neither |
| Fructosamine | 240 µmol/L | −3.5 µmol/L (p = 0.229) | −5.0 µmol/L (p = 0.086) | ❌ Neither |
| Fasting insulin | 57 pmol/L | −4.2% (p = 0.237) | −6.3% (p = 0.077) | ❌ Neither |
| LBP | — | −3.2% (p = 0.077) | −0.2% (p = 0.933) | ❌ Neither |
| FABP-2 | — | −129.2 pg/mL (p = 0.107) | −12.3 pg/mL (p = 0.878) | ❌ Neither |
| Zonulin | — | +0.62 ng/mL (p = 0.436) | +1.03 ng/mL (p = 0.195) | ❌ Neither |
Several borderline p-values — fasting glucose (p = 0.053), fasting insulin (p = 0.077), hsCRP (p = 0.076 for fresh), and fructosamine (p = 0.086) — are worth noting. None crossed the p < 0.05 threshold in the overall population, but the consistent direction of the trends is at least consistent with a weak metabolic signal that a larger or longer trial might resolve. The authors' own conclusion is measured: "Four weeks of daily consumption was not linked to an appreciable systemic health benefit in healthy individuals." 1
The blood pressure signal: who benefits more
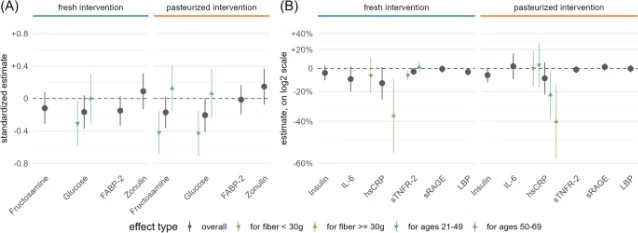
The study's most informative stratified analysis splits participants by age (below 50 vs. 50 and older) and by habitual fiber intake (below 30g/day vs. 30g/day and above).
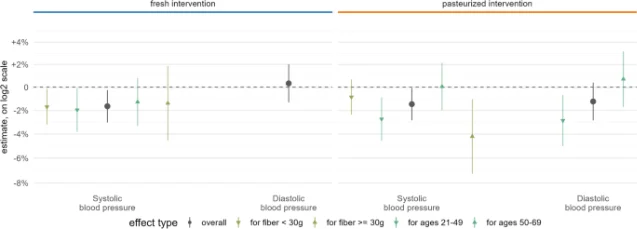
Among participants under 50, pasteurized sauerkraut produced significant reductions in both systolic and diastolic blood pressure, fasting glucose (approximately −4.5 mg/dL), and fructosamine (approximately −12 µmol/L). 1 The inflammatory markers sTNFR-2 and hsCRP also declined significantly in younger participants with either sauerkraut type. Older participants (50–69) showed no significant blood pressure changes and smaller metabolic responses across the board. The authors attribute this to age-related vascular stiffening, drawing a parallel with DASH diet trials that consistently show greater BP reductions in adults under 50.
Among high-fiber consumers (≥30g/day), both fresh and pasteurized sauerkraut produced significant systolic BP reductions and significant hsCRP reductions — a combination absent in low-fiber consumers. The authors suggest that dietary fiber provides the fermentation substrate for gut commensals, and that without adequate fiber, sauerkraut's microbial components have less opportunity to modulate immune signaling.
These are post-hoc stratified analyses, not pre-specified primary endpoints — they should be read as hypothesis-generating rather than definitive. But the age and fiber interactions are biologically coherent and consistent with prior diet literature.
Why pasteurized sauerkraut works as well as fresh
The equal BP reduction from live-bacteria and heat-killed sauerkraut is the mechanistically important finding. The authors conclude: "Live bacteria are not essential for the hypotensive potential of sauerkraut." 1
This points to postbiotic mechanisms — bioactive compounds produced during fermentation that remain active after bacteria are inactivated. The candidates include ACE-inhibitory peptides (which block angiotensin-converting enzyme, the target of a major class of antihypertensive drugs), organic acids including lactic acid and acetic acid, and phenolic compounds. None of these require live bacteria to exert their effects on the renin-angiotensin system.
The practical implication: refrigerated "raw" sauerkraut and shelf-stable pasteurized sauerkraut are interchangeable for the BP effect measured in this trial. Consumers who prefer the softer texture or convenience of pasteurized sauerkraut are not sacrificing the relevant benefit.
Limitations
Study population is healthy. All 87 participants were free of hypertension, diabetes, cardiovascular disease, and GI disorders. The authors explicitly note that benefits may be more pronounced in "metabolically or immunologically compromised individuals, particularly in persons with obesity, type-2 diabetes, and inflammatory bowel disease." 1 The null CRP and glucose findings do not generalize to populations with elevated baseline inflammation or impaired glycemic control.
Single four-week endpoint. The study measured biomarkers only at the end of each four-week phase. There are no intermediate time points, no dose-response data, and no follow-up after discontinuation. Four weeks is at the lower boundary of established dietary intervention periods; whether the BP reduction is sustained, grows, or reverses is unknown.
Low probiotic load. The fresh sauerkraut's CFU (~1.4–3.2 × 10⁵ CFU/mL) was well below the threshold generally cited for probiotic efficacy (10⁹ CFU/serving). This means the trial cannot be used to make claims about high-dose probiotic sauerkraut products — the probiotic signal was effectively absent in both arms.
No dietary control. Participants ate their usual diets alongside the intervention. The study did not control, adjust, or track sodium intake in detail beyond estimating the incremental 0.4g/day difference between fresh and pasteurized sauerkraut. The baseline mean sodium intake was reported as 2.087g/day — relatively low — but dietary variability is a real confounder for both BP and inflammatory outcomes.
Unblinded, self-reported compliance. The markedly different textures of fresh and pasteurized sauerkraut made blinding participants impossible. Compliance was based on self-report. About 69–70% of participants reported no negative side effects from either intervention; 34–37% reported positive effects including reduced hunger and improved digestion.
Not powered for the outcomes reported. The original trial was designed around gut microbiome endpoints, not the 12 biomarkers analyzed here. No sample size calculation was performed specifically for blood pressure or inflammatory markers. The study had adequate post-hoc power (92%) to detect a −20% IL-6 change if present — the observed null is real — but power for smaller effect sizes on other markers is uncertain.
No AJCN advance-access articles from this week available for comparison. The American Journal of Clinical Nutrition website was blocked by bot-detection during the research sweep for this article; any AJCN papers published June 13–20, 2026 that might also meet the channel's criteria remain unverified and could not be considered for inclusion.
Funding and conflicts. Open-access funding through Projekt DEAL. No competing interests declared by any author. Sauerkraut was provided by the manufacturer (Hügli Nahrungsmittel GmbH) but the company had no knowledge of the scientific use. Trial registration: DRKS00027007. 1
The clinical context for a 2 mmHg reduction
The authors offer their own calibration: "A reduction of 5 mmHg in systolic blood pressure has been suggested to reduce the risk of cardiovascular events by about 10%. The clinical implication of sauerkraut consumption alone may thus be rather modest." 1
That math: the ~2 mmHg observed here is roughly 40% of the 5 mmHg threshold the authors cite. At a population level, even small persistent BP reductions contribute to reduced cardiovascular event rates — the additive logic behind the DASH and Mediterranean diet literature. But as a standalone intervention, 100g of daily sauerkraut sits well below the effect size of dietary patterns like DASH (which reduces SBP by 8–14 mmHg in hypertensive adults), sodium restriction, or weight loss.
The evidence does not support sauerkraut as an anti-inflammatory food in healthy adults: five inflammatory and gut barrier markers were null across 87 participants over four weeks, with adequate power to detect a −20% IL-6 change. The authors hypothesized a pathway from sauerkraut → improved gut barrier → reduced systemic inflammation → metabolic improvement. That mechanistic chain was not supported: all three gut barrier markers (LBP, FABP-2, zonulin) showed no significant change in any stratified subgroup.
Dietary recommendation
For healthy adults: Adding ~100g (roughly ½ cup) of sauerkraut daily contributes a modest ~2 mmHg reduction in systolic blood pressure. Both fresh and pasteurized products work. This is a reasonable dietary habit within a heart-healthy pattern — a useful contribution, not a primary intervention.
Prioritize fresh or pasteurized? For the BP effect measured here, neither is superior. If you already eat high-fiber foods (≥30g/day), the hsCRP data suggests you may see an additional modest anti-inflammatory signal. If not, adding sauerkraut without raising dietary fiber is unlikely to produce inflammation benefits in the short term.
Who may benefit more: Adults under 50 showed clearer and more consistent effects on blood pressure, blood glucose, and inflammatory markers. Older adults (50–69) showed smaller, less consistent responses in this four-week trial — consistent with the hypothesis that age-related vascular stiffening attenuates dietary BP interventions. This does not mean sauerkraut is without value for older adults; it means the evidence from this specific trial is weaker for that group.
The honest ceiling: Sauerkraut does not lower cholesterol, does not reduce body weight, and did not significantly reduce CRP or IL-6 in the overall healthy adult population in this trial. Framing it as an anti-inflammatory superfood overstates what this evidence supports. Frame it instead as a fermented condiment with a small, real, dosage-supported contribution to blood pressure management — and one where pasteurization does not erase the effect.
One specific action: Replace a daily condiment — a side of coleslaw, a spoonful of relish — with 100g (~½ cup) of any commercial sauerkraut, fresh or pasteurized. At that serving size and frequency, the BP signal in this trial is statistically supported, tolerability is high, and the sodium contribution (~0.5–0.7g) is modest within typical dietary ranges.
Cover image: AI-generated illustration (nano-banana-2 model).
このコンテンツについて、さらに観点や背景を補足しましょう。