Highest vs. lowest PHD adherence: summary estimates
Khuc et al., Preventive Medicine 2026 · 23 prospective cohort studies · NutriGrade moderate-to-high · Exact HRs with 95% CI unavailable (full text paywalled)

A June 2026 Bayesian dose-response meta-analysis in Preventive Medicine (Khuc et al., 23 prospective cohort studies) finds that mortality and CVD risk reductions from the EAT-Lancet Planetary Health Diet begin at moderate adherence — not only at the highest tier — with 17% lower all-cause mortality, 16% lower cardiovascular mortality, and 18% lower total CVD risk at highest vs. lowest adherence. Myocardial infarction showed no significant association. The concrete takeaway: a plant-heavy daily pattern with whole grains, legumes, vegetables, and nuts — and red meat capped at one serving per week — is enough to sit in the part of the dose-response curve where risk is meaningfully lower.

リサーチノート
"Expanding on previous studies that focused on highest versus lowest adherence groups, we found that significant reductions in the risks of all-cause mortality, cardiovascular mortality, total CVD, and several CVD subtypes were observed starting from at least moderate adherence to the PHD." 2
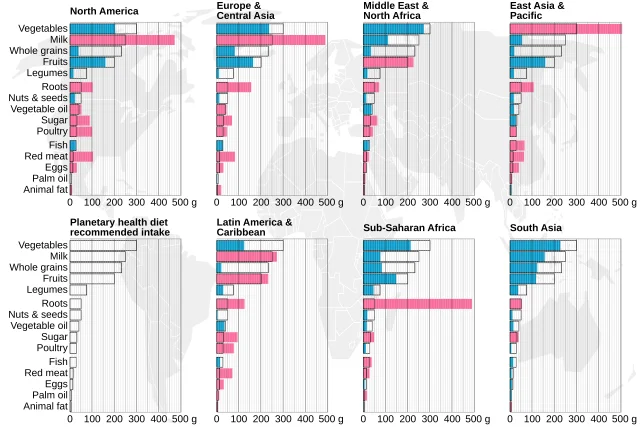
| Food group | Daily target | Practical equivalent |
|---|---|---|
| Whole grains | 232 g | ~1.5 cups cooked brown rice, or ~3 slices whole-grain bread |
| Vegetables | 300 g | ~4 cups raw leafy greens, or 2 cups mixed cooked vegetables |
| Fruits | 200 g | ~1.5 medium apples, or 1.5 cups berries |
| Legumes (dry weight) | 75 g | ~½ cup cooked lentils or chickpeas |
| Nuts | 50 g | ~1.5 oz, a small handful of mixed nuts |
| Red meat (beef/lamb/pork) | ≤14 g/day (≤98 g/week) | ~1 small hamburger patty per week |
| Poultry | 29 g | ~1 boneless chicken thigh every other day |
| Fish | 28 g | ~2 palm-sized servings per week |
| Eggs | 13 g | ~1 egg every third day |
| Dairy | 250 g | ~1 cup milk or yogurt |
| Unsaturated oils | 40 g | ~3 tablespoons olive oil |
| Added sugars | ≤31 g | ~2 tablespoons honey or ~8 teaspoons sugar |
このコンテンツについて、さらに観点や背景を補足しましょう。