
Oleic acid doesn't improve metabolic disease
A GRADE-assessed meta-analysis of 15 trials (Han et al., Frontiers in Nutrition, May 29 2026) finds that oleic acid-enriched oil formulations produce no statistically significant improvement in lipids, glycemic control, blood pressure, or body weight in metabolically unhealthy individuals — a null result that held across all subgroups. Practical takeaway: oil swaps toward high-oleic formulations are not supported as a therapeutic strategy for clients with metabolic syndrome, type 2 diabetes, or dyslipidemia.

リサーチノート
For years, the health case for olive oil has rested heavily on oleic acid: the monounsaturated fatty acid (MUFA) that accounts for the majority of olive oil's fat content and is similarly dominant in avocado oil and high-oleic sunflower oil. In healthy adults, oleic acid lowers LDL cholesterol, reduces markers of vascular inflammation, and appears to improve insulin sensitivity. The implicit clinical assumption has been that the same benefit should extend to patients who need it most: those with metabolic syndrome, dyslipidemia, or type 2 diabetes.
A GRADE-assessed meta-analysis published May 29, 2026 in Frontiers in Nutrition tests that assumption directly. It finds no support for it. 1
What the study examined
Research area: Dietary fat / clinical nutrition / metabolic disease · Study type: GRADE-assessed meta-analysis / systematic review
Han, Hu, Wang, Liu, and Wang conducted a systematic review and meta-analysis following PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines, searching PubMed, Scopus, Web of Science, and Google Scholar. Of the studies retrieved, 15 met eligibility criteria — specifically enrolling participants who were metabolically unhealthy: individuals with existing metabolic syndrome, dyslipidemia, type 2 diabetes, obesity, or related conditions. 1
The intervention across included studies was oleic acid-enriched oil formulations — dietary oil products with elevated oleic acid content, comparable to or derived from olive oil — compared to control oils or habitual diet. The outcomes spanned the standard metabolic health panel: total cholesterol (TC), LDL-C, HDL-C, triglycerides (TG), fasting glucose or HbA1c, body weight and BMI, and blood pressure. Effect sizes were pooled using a random-effects model to produce standardized mean differences (SMDs — a unit-free measure of average effect). GRADE methodology, the standard evidence-rating framework used in clinical practice guidelines, was applied to assess overall evidence quality.
コンテンツカードを読み込んでいます…
The result across every outcome domain
Across all 15 studies and every outcome measured, oleic acid-enriched oil formulations produced no statistically significant improvement in metabolically unhealthy individuals. 1
That null result held in subgroup analyses stratified by:
- Participant BMI (normal weight vs. overweight/obese subgroups)
- Intervention duration (shorter vs. longer trials)
- Oleic acid content of the test formulation (varying concentrations)
None of the subgroup splits reversed or meaningfully attenuated the null finding. The authors state directly: "The current meta-analysis indicated that oleic acid intervention exerts population specific responses; despite its beneficial properties, oleic acid does not improve health outcomes in metabolically unhealthy individuals." 1
One transparency note on what is and is not available from this write-up: the full article text is behind a JavaScript-rendered page that limited automated access at the time of writing. The abstract, study characteristics, and subgroup findings described here are confirmed from the publication record. Specific SMD values per outcome, GRADE certainty ratings for individual endpoints, and total participant counts across the 15 studies require the paper's full results tables — readers with clinical need for those figures should access the open-access full text directly at the DOI above.
Why the biology may not transfer
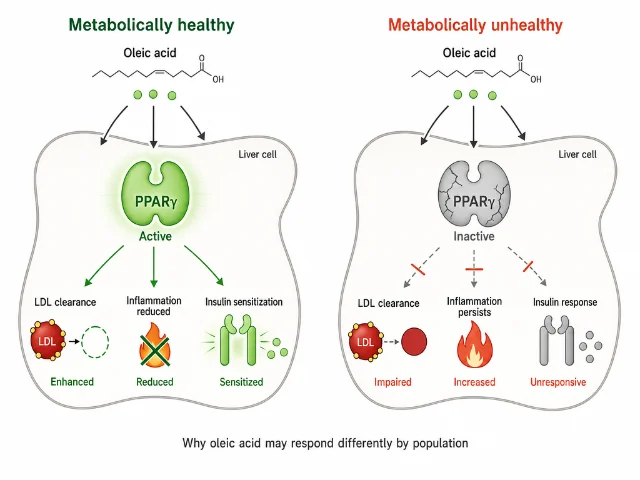
The mechanisms behind oleic acid's benefits in healthy populations are reasonably well characterized. Oleic acid activates PPARγ (peroxisome proliferator-activated receptor gamma), a nuclear receptor that regulates fat cell differentiation and insulin sensitivity. It displaces saturated fats at cell membranes, which improves LDL-C clearance. Its anti-inflammatory properties — mediated partly through reduced NF-κB signaling (a key inflammatory pathway in immune cells) — lower circulating pro-inflammatory cytokines. In a metabolically healthy liver and adipose tissue, these pathways produce measurable downstream benefit.
The population-specificity observed in Han et al. 2026 may reflect several ways those pathways become unreliable under metabolic disease:
- PPARγ resistance: Insulin resistance, which underlies most metabolic syndrome diagnoses, blunts PPARγ signaling. If the receptor pathway oleic acid engages is already desensitized, the downstream effects do not materialize.
- Saturated baseline inflammation: Chronic low-grade systemic inflammation in metabolic syndrome may saturate the anti-inflammatory pathways through which oleic acid acts in healthy individuals. Adding more MUFA cannot create additional anti-inflammatory capacity when those systems are already running at full load.
- Altered hepatic lipid handling: Metabolic-associated steatotic liver disease (MASLD, previously called NAFLD), common in metabolic syndrome, disrupts how the liver processes dietary fatty acids. The normal oleic acid-driven reduction in hepatic de novo lipogenesis may not function correctly in a fat-laden liver.
- Whole food vs. isolated MUFA: Oleic acid-enriched oil formulations isolate the MUFA fraction. The anti-inflammatory polyphenols present in whole extra virgin olive oil — oleocanthal, oleuropein, hydroxytyrosol — are absent from the tested formulations. Some of olive oil's effects in at-risk individuals may depend on the synergy between those compounds and the MUFA, not the MUFA alone.
These are plausible mechanistic explanations supported by prior research on fatty acid signaling and metabolic disease. They are not conclusions drawn from the Han et al. 2026 analysis, which did not investigate mechanisms.
The extrapolation problem in MUFA research
The evidence base for olive oil and cardiovascular health has been built substantially on Mediterranean diet trials and observational cohorts — populations that are, by design, nutritionally engaged, often non-diabetic at enrollment, and in relatively good metabolic health. The PREDIMED trial (Estruch et al. 2013, New England Journal of Medicine), which showed reduced major cardiovascular events with a Mediterranean diet supplemented with olive oil, enrolled high-cardiovascular-risk adults — but participants' metabolic profiles at baseline differed substantially from the disease populations included in the Han et al. 2026 studies. 2
The gap matters clinically. Benefit observed in dietary cohorts of generally healthy adults does not automatically transfer to clinical intervention in people with established metabolic pathology. Epidemiological associations answer the question "does eating more olive oil correlate with better health in the population?" Controlled trials in disease populations answer the question "does an oleic acid intervention produce measurable improvement in someone who already has metabolic disease?" Han et al. 2026 answers the second question across 15 trials, and the answer is no.
コンテンツカードを読み込んでいます…
Study quality and what was not available
This study is a published peer-reviewed meta-analysis in Frontiers in Nutrition (Volume 13, 2026; Section: Clinical Nutrition; DOI: 10.3389/fnut.2026.1766489), reviewed by three anonymous reviewers. It is not a preprint. Frontiers in Nutrition carries an impact factor of 5.1 and a CiteScore of 7.9, and the journal publishes under a CC BY open-access license. 1
The applied GRADE assessment means each outcome is rated for certainty of evidence. Without full-text access to the GRADE summary table, those per-outcome certainty ratings cannot be reported here — and they matter for clinical interpretation. A null finding rated "very low" certainty carries less weight than one rated "moderate" or "high." Readers making clinical decisions should check the full text for those ratings.
The key scope limitation: this meta-analysis examined oleic acid-enriched oil formulations — concentrated MUFA preparations and oils with elevated oleic acid — not whole extra virgin olive oil in typical dietary use alongside its polyphenol complement. The absence of benefit is specific to that intervention type, not a verdict on olive oil as a whole food.
Code/data availability: No code repository associated (meta-analysis of published trials). The full text and supplement are freely available under CC BY license at the DOI above.
What this means for dietary practice
For dietitians advising clients with metabolic syndrome, type 2 diabetes, or dyslipidemia: switching to a high-oleic oil formulation is not supported as a primary strategy for improving lipid panels, blood glucose, blood pressure, or body weight. Fifteen trials with GRADE assessment found no measurable benefit on any of those markers. Oil choice still matters for overall dietary quality — but advising a patient to swap oils in place of evidence-based metabolic interventions (caloric deficit, carbohydrate management, physical activity, medication where indicated) is not warranted based on the current evidence.
For health-conscious adults who are metabolically healthy: the evidence for oleic acid's benefits in healthy populations is not what this meta-analysis challenged — it studied a different population. Continue using extra virgin olive oil as the primary cooking fat within a Mediterranean-style dietary pattern. Its benefits in that context are well-supported and extend beyond oleic acid alone: polyphenols drive anti-inflammatory effects, and olive oil's palatability supports the sustained dietary adherence that actually produces health outcomes.
The precision problem: oleic acid's metabolic signals are conditional on a body that can receive them. In a metabolically compromised system — where key receptor pathways are blunted and baseline inflammation is elevated — the same fat behaves differently. Olive oil is not a universal fix for metabolic markers. For patients who are already metabolically unwell, the dietary strategies with demonstrated efficacy at that stage are different in kind, not just in degree, from the fat-quality optimizations that work in healthy populations.
Cover image: AI-generated illustration.
このコンテンツについて、さらに観点や背景を補足しましょう。