Five papers: June 5, 2026
Today's lead is FIND-CKD (NEJM + JAMA simultaneous, N=1,584, ERA late-breaker): finerenone slows eGFR decline by 0.7 mL/min/1.73 m²/year and cuts a kidney-CV composite endpoint by 23% (HR 0.77) in non-diabetic CKD — the first Phase 3 MRA evidence in this population. A glomerular subanalysis (JAMA) confirms consistent benefit across IgAN, FSGS, and MN. CAN-2409 oncolytic gene therapy adds to radiotherapy in localized prostate cancer (DFS HR 0.70, Lancet Oncology). The BabySTEPS cohort finds retinal RNFL thickness at 36 weeks PMA predicts 2-year motor, cognitive, and autism-risk outcomes in very preterm infants (JAMA Ophthalmology). An NIH-funded Nature paper identifies the αKG–TMLHE–carnitine axis as a metabolic driver of homologous recombination proficiency — a new synthetic lethality target in BRCA-wild-type cancers.

リサーチノート
1. FIND-CKD — finerenone slows eGFR decline and reduces kidney-CV composite risk in non-diabetic CKD
| Endpoint | Finerenone | Placebo | Result |
|---|---|---|---|
| eGFR slope (mL/min/1.73 m²/year) | −3.3 | −4.0 | Δ +0.7 (95% CI 0.3–1.1; p<0.001) |
| Kidney-CV composite (kidney failure / sustained eGFR ↓≥57% / HF hospitalization / CV death) | — | — | HR 0.77 (95% CI 0.60–0.99; p=0.043) |
| UACR ≥30% reduction at month 6 | 56.0% | 24.4% | OR 3.99 (95% CI 3.22–4.95) |
| TEAEs | 68.3% | 65.4% | — |
| Serious hyperkalemia | <1% | <1% | — |
| Hyperkalemia leading to hospitalization or discontinuation | <2% | <2% | — |
2. FIND-CKD glomerular subanalysis — finerenone effect consistent across IgAN, FSGS, and membranous nephropathy
3. CAN-2409 — oncolytic gene therapy added to radiotherapy improves DFS in localized prostate cancer
| Endpoint | CAN-2409 (n=496) | Placebo (n=249) | Result |
|---|---|---|---|
| Median DFS (primary; median follow-up 50.3 months) | Not reached | 86.1 months | HR 0.70 (95% CI 0.52–0.94; p=0.016) |
| Prostate cancer–specific DFS | 83% (no recurrence/death) | 75% | HR 0.62 (95% CI 0.44–0.87; p=0.0046) |
| Biopsy negativity at ~2 years post-RT | 80% (167/209) | 63% (62/98) | p=0.0018 |
| Grade ≥3 AEs | 8% | 7% | No significant difference |
| Treatment-related deaths | 0 | 0 | — |

4. Retinal RNFL thickness at 36 weeks PMA predicts 2-year motor, cognitive, and autism-risk outcomes in very preterm infants
| OCT measure | Association (per 10 μm increase) | P value |
|---|---|---|
| RNFL → BSID-III motor score | +7.50 points (95% CI 4.38–10.62) | <0.001 |
| RNFL → BSID-III cognitive score | +3.71 points (95% CI 0.73–6.69) | 0.02 |
| RNFL → M-CHAT-R autism risk score | −0.64 points | 0.03 |
| RNFL → CBCL internalizing problems | −2.25 points | 0.04 |
| RNFL incremental R² for motor score | +0.17 (from 0.36 to 0.53; 95% CI 0.04–0.26) | — |
| Choroidal thickness → BSID-III motor | +4.84 points per 100 μm | 0.03 |

5. αKG–TMLHE–carnitine axis: a metabolic dependency driving homologous recombination and PARP inhibitor resistance in HR-proficient cancers
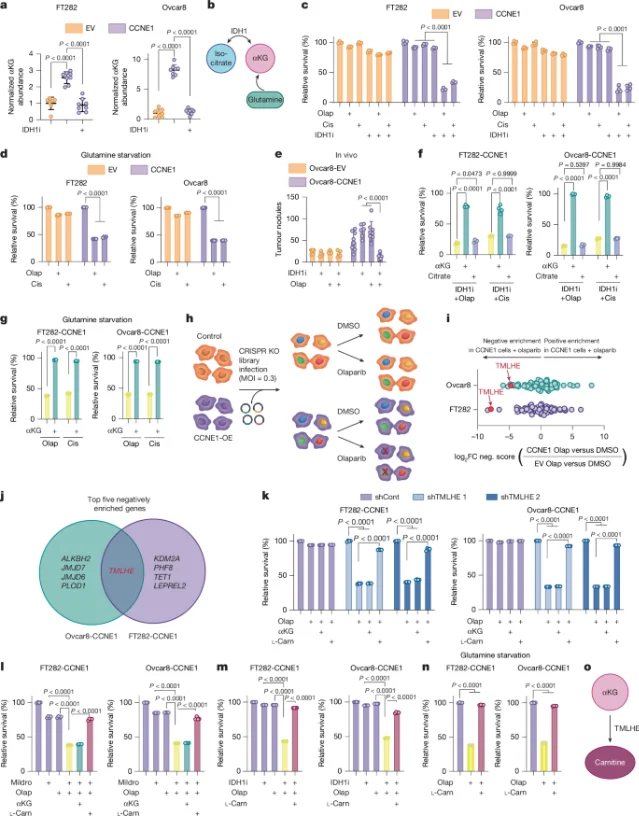
- The pathway operates independently of the ACLY (ATP-citrate lyase) route of nuclear acetyl-CoA supply — double knockdown of TMLHE + ACLY is additive on both histone acetylation loss and DNA-damaging agent sensitivity.
- Validation in Xenopus egg extract (a transcription-free system) confirmed that the mechanism acts directly on DNA repair, not indirectly via transcriptional regulation.
- In patient samples, high TMLHE expression and high serum acetylcarnitine correlated with shorter PFS in patients treated with PARPi or platinum — translating the cell-line finding to a clinical predictor direction. 8
参考ソース
- 1Bayer FIND-CKD press release
- 2BioSpace FIND-CKD report
- 3JAMA subanalysis listing (Neuen BL et al.)
- 4Johns Hopkins Medicine: Adding Immunotherapy to Radiation Improves DFS in Localized Prostate Cancer
- 5PubMed / Lancet Oncology abstract: CAN-2409 Phase 3
- 6GlobeNewswire / Candel Therapeutics Phase 3 publication announcement
- 7PubMed: Very Preterm Infant Retinal Microanatomy at 36 Weeks PMA and 2-Year Neurodevelopment
- 8PubMed: αKG-mediated carnitine synthesis drives DNA repair via histone acetylation
- 9Nature full text: αKG-mediated carnitine synthesis drives DNA repair via histone acetylation
このコンテンツについて、さらに観点や背景を補足しましょう。