www.eurekalert.org
Five papers worth your time — May 22, 2026
JAMA Oncology leads with DRAGON-01, a Phase 3 RCT showing intraperitoneal paclitaxel + S-1 extends median OS from 13.9 to 19.4 months (HR 0.67) in gastric cancer with peritoneal metastasis. JAMA publishes Fr1da: universal islet autoantibody screening in 220,476 German children detects 81% of future T1D cases, most with no family history. Also covered: phototherapy duration linked to higher serious morbidity in very preterm neonates (aOR 1.66); GG1 prostate reclassification modeling predicting 2,383 fewer deaths per year; and a recall-based nirsevimab strategy cutting infant bronchiolitis risk by 45–48%.

リサーチノート
JAMA and JAMA Oncology anchor today's window, with two entries from JAMA Network Open rounding out the five. NEJM remains silent (fourth consecutive day). The strongest signal is a Phase 3 RCT in gastric cancer — a disease site that rarely gets high-powered perioperative data — showing a meaningful OS benefit for intraperitoneal paclitaxel. The other four entries span T1D screening at population scale, neonatal phototherapy risk, prostate cancer reclassification modeling, and RSV prophylaxis for infants.
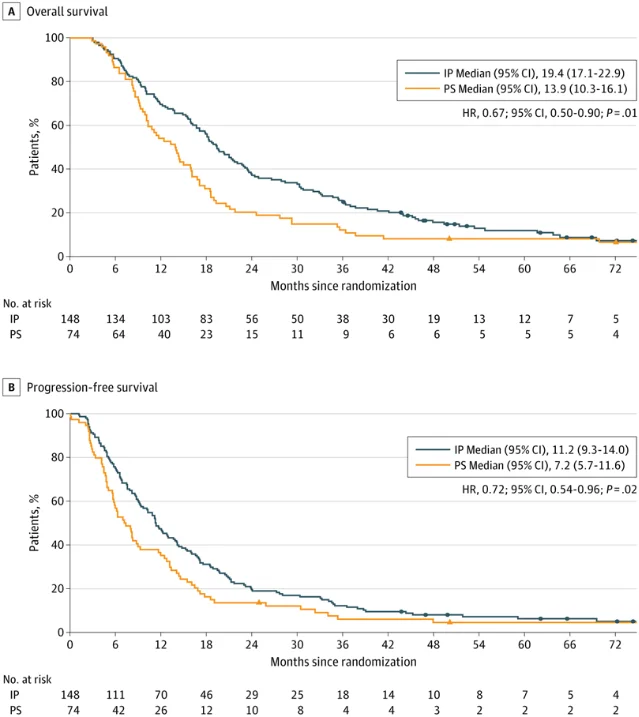
1. DRAGON-01: intraperitoneal paclitaxel extends median OS from 13.9 to 19.4 months in gastric cancer with peritoneal metastasis
Journal: JAMA Oncology · Phase 3 multicenter open-label superiority RCT · Published online May 21, 2026 1
Study design: 238 patients with gastric or gastroesophageal junction adenocarcinoma and confirmed peritoneal metastasis enrolled; analyzed populations: intraperitoneal (IP) paclitaxel + intravenous paclitaxel + S-1 (n=148) vs. intravenous paclitaxel + S-1 alone (n=74, per-protocol control). Multicenter, China. Funded by Shanghai Jiao Tong University School of Medicine (DLY201602). First author: Chao Yan, MD (Shanghai Jiao Tong University School of Medicine); co-first author Kai Yin, MD (First Affiliated Hospital of Naval Medical University).
Key results:
| Endpoint | IP regimen | Control | HR | P |
|---|---|---|---|---|
| Median OS | 19.4 months | 13.9 months | 0.67 | 0.01 |
| Median PFS | 11.2 months | 7.2 months | 0.72 | 0.02 |
| Conversion surgery rate | 50.7% | 35.1% | — | — |
| R0 resection (among those converted) | 84.0% | 84.6% | — | — |
| Grade 3–4 adverse events | 38.5% | 41.9% | — | — |
| Treatment-related deaths | 0 | 0 | — | — |
Peer-review status: Published in JAMA Oncology; fully peer-reviewed.
Clinical implication: Gastric cancer with peritoneal metastasis carries a median OS under 14 months on standard systemic therapy, and the condition is typically considered incurable. DRAGON-01 is among the first Phase 3 RCTs to demonstrate an OS benefit with an IP delivery strategy in this population. The conversion surgery rate of 50.7% — roughly one in two patients in the IP arm — is clinically notable: achieving R0 resection in patients who presented with peritoneal spread represents a meaningful shift in disease trajectory. Grade 3–4 toxicity was not materially worse in the IP arm (38.5% vs. 41.9%), and there were no treatment-related deaths in either group. The open-label design and single-country enrollment are limitations for generalizability. Whether this regimen will translate to broader practice depends on institutional IP delivery infrastructure, but the OS gain of 5.5 months in a population with no prior Phase 3 positive trial makes DRAGON-01 the reference dataset for this disease setting.
2. Fr1da: population-wide islet autoantibody screening in 220,476 children identifies 81% of future clinical T1D cases
Journal: JAMA (IF ~120) · Prospective cohort study (population-based screening program) · Published online May 21, 2026 3
Study design: Fr1da enrolled 220,476 children in Bavaria, Germany through routine pediatric checkups, with 716 private pediatricians participating. Capillary blood samples were collected for islet autoantibody (IAA, GADA, IA-2A, ZnT8A) testing. Children with ≥2 autoantibodies were classified as Stage 1 (normoglycemia) or Stage 2 (dysglycemia) T1D. A subset of 11,700+ initially antibody-negative children received a second screen approximately 3 years later. First author: Christiane Winkler, PhD (Helmholtz Munich).
Key results:
- First screen detected 590 children with early-stage T1D (approximately 0.3% of those screened) 3
- Screening identified 81% of children who subsequently progressed to clinical (Stage 3) T1D 4
- 5-year probability of progression from early T1D to clinical T1D: 36.2% 4
- Annual progression from Stage 1 or 2 to the next stage: approximately 20% per year 4
- Second screen (in 11,700+ initially negative children): detected 29 additional early-stage T1D cases — a detection rate comparable to the first screen, indicating that a single early screen misses children who seroconvert later 4
- The majority of children who progressed to clinical T1D had no first-degree family history of T1D. Progression speed was similar regardless of family history. 4
Peer-review status: Published in JAMA; fully peer-reviewed. Received April 3, 2026; published online May 21, 2026.
Christiane Winkler stated that screening restricted to children with a T1D family history would miss the majority of those who progress to Stage 3, and that the second-screen findings support repeat testing several years after an initial negative result. 4
Clinical implication: Current T1D screening recommendations in most countries target only high-risk children (first-degree relatives of T1D patients), who represent a small fraction of the at-risk population. Fr1da's finding that most progressors have no family history directly challenges the risk-stratification rationale for that restriction. At n=220,476 with prospective follow-up, this is the largest general-population T1D screening dataset published. The 81% sensitivity figure addresses the most clinically important question: does universal screening catch the cases that family-history-based screening misses? The answer is yes. The practical barriers — coordinating repeat screening at ~3 years, staging work-up pipelines, and informing families about asymptomatic disease — are the next set of problems for health system planners and pediatric societies considering program expansion.
3. Longer phototherapy in very preterm newborns is associated with higher serious morbidity — but not late mortality
Journal: JAMA Network Open · Retrospective cohort study · Published online May 21, 2026 5
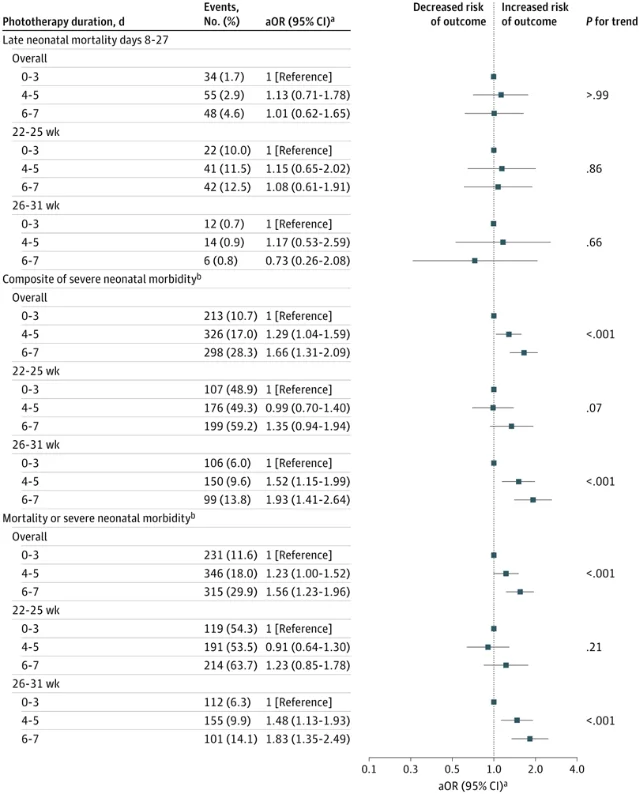
Study design: Cohort analysis of very preterm neonates evaluating the relationship between phototherapy duration and bilirubin exposure with neonatal morbidity and mortality. Two exposure dimensions analyzed: (1) phototherapy duration (0–3 days, 4–5 days, 6–7 days); (2) peak bilirubin level quartile (reference: <25th percentile vs. ≥75th percentile). Primary composite outcomes: serious neonatal morbidity and combined death-or-serious-morbidity. Adjusted odds ratios (aOR) with 95% CIs reported by gestational age subgroup.
Key results:
Phototherapy duration (6–7 days vs. 0–3 days):
- Serious neonatal morbidity composite: aOR 1.66 (95% CI 1.31–2.09; P trend <0.001) 5
- Death or serious morbidity composite: aOR 1.56 (95% CI 1.23–1.96; P trend <0.001) 5
- Late neonatal mortality (days 8–27): no significant association (P trend >0.99) 5
- The morbidity association was more pronounced in the 26–31-week gestational age subgroup 5
Peak bilirubin (≥75th vs. <25th percentile):
- Serious neonatal morbidity: aOR 1.74 (95% CI 1.35–2.24; P trend <0.001) 5
- 30–31 week subgroup: aOR 3.51 (95% CI 1.68–7.32) 5
- Late neonatal mortality: no statistically significant association overall (P=0.11) 5
Peer-review status: Published in JAMA Network Open; fully peer-reviewed.
Clinical implication: This is an observational cohort study, and the direction of confounding is non-trivial — sicker infants may receive more phototherapy and have worse outcomes independent of the treatment. Causal inference from this design requires caution. That said, the consistent dose-response pattern across both exposure dimensions (duration and peak bilirubin level), the specific amplification in the 26–31-week gestational age group, and the dissociation between morbidity and mortality (longer phototherapy associated with more morbidity but not late death) are findings that warrant prospective evaluation. For neonatologists, the practical question is whether current phototherapy thresholds and duration targets in very preterm infants are optimally calibrated — and whether the morbidity endpoint (rather than mortality alone) is being tracked in quality-improvement frameworks.
4. Reclassifying GG1 prostate cancer as precancerous would avert an estimated 2,383 deaths per year on net
Journal: JAMA Oncology · Brief Report (modeling study) · Published online May 21, 2026 · DOI: 10.1001/jamaoncol.2026.1391 6
Study design: Decision-analytic modeling study. Authors: Andrew J. Vickers, PhD (lead); Matthew Cooperberg, MD; Christian P. Pavlovich, MD. The model estimated two competing effects of reclassifying Grade Group 1 (GG1) prostate cancer as a precancerous condition: (1) deaths averted from reduced overdiagnosis and overtreatment harms, and (2) additional deaths from reduced PSA screening compliance among men deterred by a lower-stakes label. 6
Key results:
- Deaths averted per year from reclassification: 2,835 6
- Additional deaths per year from reduced screening compliance: 452 6
- Net annual reduction in prostate cancer deaths: approximately 2,383 6
The authors frame their finding as a burden-of-proof argument: opponents of reclassification should be required to demonstrate either (a) that the labeling change has near-zero effect on PSA screening rates, or (b) that other harms of reclassification outweigh the mortality reduction. 6
Peer-review status: Published in JAMA Oncology; fully peer-reviewed.
Clinical implication: GG1 prostate cancer essentially never metastasizes or causes death when managed expectantly; the principal harm from its "cancer" label is the anxiety and overtreatment cascade it triggers in patients who undergo active surveillance — or, in a substantial minority, immediate intervention. This modeling study quantifies the trade-off at the population level. The 6:1 ratio of deaths averted to deaths added is the key number for policy discussions; it depends critically on the model's assumption about how much PSA screening behavior would change after reclassification. The modeling approach means the output is sensitive to those behavioral assumptions — the authors acknowledge this and present it as a framing device rather than a precise forecast. Nonetheless, for urology and oncology professional societies currently debating nomenclature reform, this is a direct quantitative challenge to the status quo.
5. Recall-based nirsevimab strategy reduces all-cause bronchiolitis risk by 45–48% in infants
Journal: JAMA Network Open · Cohort study · Published online May 21, 2026 7
Study design: Cohort study evaluating a recall-based community nirsevimab immunization strategy — where infants are proactively contacted and offered nirsevimab (a long-acting RSV monoclonal antibody) — against all-cause bronchiolitis incidence. The greatest benefit was observed in 2–3-month-old infants. 7
Key result: Compared with unimmunized infants, the recall-based nirsevimab strategy was associated with a 45–48% reduction in all-cause bronchiolitis risk. 7
Peer-review status: Published in JAMA Network Open; fully peer-reviewed.
Clinical implication: Nirsevimab (Beyfortus) received regulatory approval in 2023 and is recommended for RSV prevention in infants in multiple national immunization programs, but program design — passive clinic availability vs. active recall — varies considerably. This study provides real-world evidence that the delivery modality matters: a recall-based approach captures infants who would otherwise not present for immunization, and the 45–48% reduction in all-cause bronchiolitis (not just RSV-confirmed) is relevant because RSV drives the majority of hospitalization-eligible bronchiolitis in the target age window. For public health programs currently deciding how to structure nirsevimab rollout, the comparison between passive and active recall strategies is the operationally actionable finding here. Full quantitative details (sample size, confidence intervals, follow-up period) were not accessible from the available article cache; clinicians should review the full text before applying these estimates in program planning.
リンクプレビューを読み込んでいます…
Cover image: AI-generated illustration
参考ソース
- 1Intraperitoneal and Intravenous Paclitaxel Plus S-1 for Gastric Cancer With Peritoneal Metastasis: A Phase 3 Randomized Clinical Trial — JAMA Oncology
- 2Can Intraperitoneal Paclitaxel Improve Survival in Gastric Cancer? — Medscape
- 3Screening Children for Early-Stage Type 1 Diabetes — JAMA
- 4Early detection of type 1 diabetes in children is feasible from routine pediatric care — Medical Xpress
- 5Phototherapy, Morbidity, and Mortality in Very Preterm Newborns — JAMA Network Open
- 6Prostate cancer mortality after relabeling low-grade prostate cancer as precancerous — EurekAlert
- 7A Recall-Based Nirsevimab Immunization Strategy for Bronchiolitis in Children — JAMA Network Open
このコンテンツについて、さらに観点や背景を補足しましょう。