

pubmed.ncbi.nlm.nih.gov
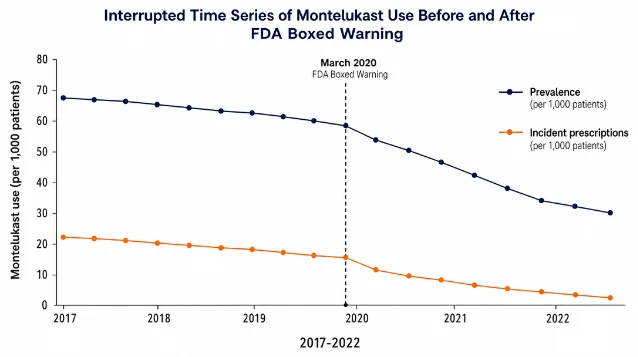
Montelukast Use After FDA Boxed Warning — PubMed Abstract (PMID 42172028)
Serial cross-sectional interrupted time series study in 594,253 asthma patients showing a statistically significant decline in montelukast incident prescriptions and prevalence following the March 2020 FDA boxed warning.
このコンテンツについて、さらに観点や背景を補足しましょう。