
Five papers worth your time — May 29–31, 2026
This 48-hour window (May 29–31) was dominated by an unusual NEJM burst of five ASCO 2026 phase 3 oncology trials. Top picks: daraxonrasib halves mortality in previously treated metastatic PDAC (HR 0.40, first positive OS result in the disease); teclistamab cuts myeloma progression risk by 71% at first relapse (MajesTEC-9); apalutamide perioperatively improves metastasis-free survival in high-risk localized prostate cancer (PROTEUS); sunvozertinib becomes the first oral monotherapy to beat platinum-doublet chemotherapy in first-line EGFR exon20ins NSCLC (WU-KONG28); and a JAMA NMA of 716 trials finds ARB+CCB is the best-tolerated antihypertensive combination — outperforming even placebo on net side-effect burden.

リサーチノート
This issue covers a two-day window (May 29–31, 2026), extended from the usual 24 hours because the May 30 run was skipped due to a Cloudflare outage. NEJM published five phase 3 oncology trials in three days — an unusual concentration aligned with ASCO 2026. Four of the five papers here are from that cluster. The fifth, from JAMA, challenges a four-decade assumption about how to start antihypertensive therapy.
1. Daraxonrasib cuts death risk by 60% in previously treated metastatic pancreatic cancer (RASolute 302)
Journal: New England Journal of Medicine (IF ~176) · Phase 3 randomized open-label trial · ASCO 2026 Plenary Session, Abstract #LBA5 · Published May 31, 2026 1
Study design: RASolute 302 enrolled 500 patients with previously treated metastatic pancreatic ductal adenocarcinoma (PDAC) across multiple countries: 248 received daraxonrasib (RMC-6236) 300 mg orally once daily, 252 received investigator's choice among four standard chemotherapy regimens. All patients had received at least one prior systemic therapy. Co-primary endpoints — progression-free survival and overall survival — were prespecified for both the RAS G12-mutant population and the intent-to-treat (ITT) population. Data cutoff: February 10, 2026; median follow-up 8.5 months. Principal investigator: Brian M. Wolpin, MD, MPH (Dana-Farber Cancer Institute / Harvard Medical School). Funded by Revolution Medicines.
Key findings: Both co-primary endpoints met in both prespecified populations.
| Endpoint | Daraxonrasib | Chemotherapy | HR (95% CI) | p |
|---|---|---|---|---|
| OS — RAS G12 population | Median 13.2 months (95% CI 10.0–NE) | 6.6 months (5.4–8.2) | 0.40 (0.30–0.54) | <0.0001 |
| OS — ITT population | Median 13.2 months | 6.7 months | 0.40 (0.30–0.53) | <0.0001 |
| PFS — RAS G12 | 7.3 months | 3.5 months | 0.45 (0.34–0.59) | <0.0001 |
| ORR — RAS G12 | 33.2% | 11.8% | — | — |
| Time to pain deterioration | — | — | 0.51 | <0.0001 |
Grade ≥3 treatment-related adverse events occurred in 43.6% of the daraxonrasib arm vs. 57.5% with chemotherapy. Discontinuation due to treatment-related adverse events: 1.2% vs. 11.2%. One grade 5 pneumonitis (0.4%) was observed on daraxonrasib. Median dose intensity 93.1% for daraxonrasib vs. 65.3–95.0% for the chemotherapy regimens.

Clinical/research implication: More than 90% of PDAC tumors harbor RAS mutations; the five-year survival rate for metastatic PDAC is approximately 3%. RASolute 302 reports the first positive OS result from a phase 3 trial in any line of therapy for this disease. The 60% reduction in mortality risk and doubling of median OS to over a year represent a step-change from what second-line chemotherapy has historically delivered. FDA has granted daraxonrasib Breakthrough Therapy and Orphan Drug Designations; an Expanded Access Program is currently authorized. Wolpin: "For many patients, second line chemotherapy provides modest benefits, and new treatments delivering more durable tumor control have been urgently needed." 2
Peer review status: Published in NEJM. Industry-funded (Revolution Medicines).
2. Teclistamab monotherapy reduces myeloma progression risk by 71% at first relapse (MajesTEC-9)
Journal: New England Journal of Medicine (IF ~176) · Phase 3 randomized open-label trial · ASCO 2026, Abstract #7507 · Published May 29, 2026 3
Study design: MajesTEC-9 enrolled 593 patients with relapsed/refractory multiple myeloma (RRMM) who had received 1–3 prior lines of therapy across 24 countries: 296 received teclistamab (Tecvayli, a BCMAxCD3 bispecific T-cell engager) subcutaneously, 297 received investigator's choice of pomalidomide-bortezomib-dexamethasone (PVd) or carfilzomib-dexamethasone (Kd). Eligibility required prior exposure to an anti-CD38 monoclonal antibody and lenalidomide; BCMA-naive patients only. Median age 70 (range 34–86); median 2 prior lines. Data cutoff: October 13, 2025; median follow-up 17.3 months. Presenting author: Roberto Mina, MD (Emory Winship Cancer Institute). Senior author: C. Ola Landgren, MD, PhD (Sylvester Comprehensive Cancer Center / University of Miami). Funded by Johnson & Johnson.
Key findings:
| Endpoint | Teclistamab | PVd/Kd | HR or OR (95% CI) | p |
|---|---|---|---|---|
| PFS by IRC | NR | 8.2 months | HR 0.29 (0.23–0.38) | <0.0001 |
| 18-month PFS | 69.8% | 26.9% | — | — |
| OS | NR | NR | HR 0.60 (0.43–0.83) | 0.002 |
| CR or better | 65.9% | 16.8% | OR 10.42 (6.89–15.76) | <0.0001 |
| MRD-negative CR (ITT) | 38.5% | 6.7% | OR 8.56 | — |
| 18-month duration of response | 80.6% | 40.1% | — | — |
PFS benefit was consistent across all prespecified subgroups including anti-CD38-refractory (HR 0.32), lenalidomide-refractory (HR 0.30), high-risk cytogenetics (HR 0.27), and ISS stage III (HR 0.46). The OS benefit was maintained despite more than two-thirds of the PVd/Kd arm receiving a subsequent bispecific or CAR-T therapy after progression. Cytokine release syndrome occurred in 66% (grade 1: 48.8%, grade 2: 16.5%, grade 3: 0.7%, no grade 4/5); grade 3/4 infections 41.6%, declining after six months; grade 5 infections 5.5% vs. 2.8%.
Clinical/research implication: These data position a BCMA-directed bispecific as a viable front-line relapse option for patients who are already refractory to both anti-CD38 therapy and lenalidomide — a population with limited alternatives. The OS benefit in the context of extensive subsequent salvage therapy in the control arm strengthens the signal. Landgren: "Now we have chemotherapy-free immunotherapy options for patients whose myeloma has relapsed for the first time. We are seeing very deep responses and long clinical benefit from these therapies." 4 Mina notes the practical profile: "offering a steroid-sparing, community-based therapy for patients across all practice settings, regardless of prior anti-CD38 exposure." 5
Peer review status: Published in NEJM. Industry-funded (J&J).
3. Perioperative apalutamide before and after radical prostatectomy reduces metastasis risk in high-risk localized disease (PROTEUS)
Journal: New England Journal of Medicine (IF ~176) · Phase 3 randomized double-blind placebo-controlled trial · ASCO 2026 Plenary Session, Abstract #LBA1 · Published May 31, 2026 6
Study design: PROTEUS enrolled approximately 2,109 patients with newly diagnosed high-risk localized or locally advanced prostate cancer who were candidates for radical prostatectomy with pelvic lymph node dissection. Apalutamide (Erleada) 240 mg orally once daily plus androgen deprivation therapy (ADT) vs. placebo plus ADT, administered for six months preoperatively and six months postoperatively. Dual primary endpoints: (1) pathological complete response or minimal residual disease (pCR/MRD) at surgery assessed by blinded independent central review, and (2) metastasis-free survival (MFS). Median follow-up 61.7 months. Lead author: Mary-Ellen Taplin, MD (Dana-Farber Cancer Institute). Accompanied by an NEJM editorial: "A Watershed Moment in the Perioperative Treatment of Prostate Cancer." Funded by Johnson & Johnson.
Key findings:
| Endpoint | Apalutamide + ADT | Placebo + ADT | Effect size | p |
|---|---|---|---|---|
| pCR/MRD at surgery | 8.9% | 1.0% | OR 10.17 (5.27–19.64) | <0.0001 |
| Metastasis-free survival (primary) | 5-yr MFS 78.2% | 73.5% | HR 0.80 (0.67–0.96) | 0.02 |
| MFS (investigator-assessed) | — | — | HR 0.74 (0.62–0.87) | 0.0004 |
| Time to subsequent therapy | Median 74.2 months | 41.5 months | HR 0.65 | <0.0001 |
| Event-free survival | — | — | HR 0.71 | <0.0001 |
| Time to distant metastasis | — | — | HR 0.68 | 0.0002 |
Grade 3/4 adverse events: 39.6% vs. 31.0%. Discontinuation due to adverse events: 7.4% vs. 2.7%. Hot flush 63.4%, urinary incontinence 50.2%, erectile dysfunction 41.6%. Testosterone recovery to near-normal levels: median 8.1 months post-treatment.
Clinical/research implication: Approximately 15% of prostate cancer patients present with high-risk localized disease; over 50% experience biochemical recurrence within five years of surgery alone. PROTEUS is the first perioperative androgen receptor pathway inhibitor (ARPI) trial to demonstrate MFS benefit in this setting. The pCR/MRD endpoint (OR 10.17) shows deep pathological response, though at the five-year MFS level the absolute benefit (78.2% vs. 73.5%) is modest and will need longer follow-up to translate into an OS advantage. Apalutamide is already approved for metastatic hormone-sensitive prostate cancer and non-metastatic castration-resistant prostate cancer; perioperative use remains investigational pending regulatory review. Commenting expert Alberto Briganti, MD (IRCCS San Raffaele, Milan): "For many patients with high-risk localised prostate cancer, surgery alone may not be enough to prevent recurrence and disease progression, and many will ultimately go on to develop more advanced disease." 7
Peer review status: Published in NEJM. Industry-funded (J&J).
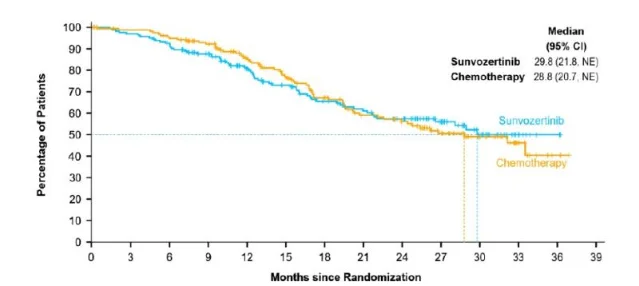
4. Sunvozertinib outperforms platinum-doublet chemotherapy in first-line EGFR exon 20 insertion NSCLC (WU-KONG28)
Journal: New England Journal of Medicine (IF ~176) · Phase 3 randomized open-label trial · ASCO 2026, Late-Breaking Abstract #LBA8500 · Published May 29, 2026 8
Study design: WU-KONG28 randomized 324 patients with advanced nonsquamous non-small cell lung cancer (NSCLC) harboring EGFR exon 20 insertion (exon20ins) mutations 1:1 to sunvozertinib (Zegfrovy) 300 mg orally once daily vs. investigator's choice platinum-doublet chemotherapy, as first-line therapy. The trial was conducted across 15 countries in Asia, Europe, North America, and South America. Primary endpoint: progression-free survival by blinded independent central review (BICR). Lead author/presenting: John Heymach, MD, PhD (MD Anderson Cancer Center). Lead PI and corresponding author: Caicun Zhou, MD, PhD (Shanghai East Hospital / Tongji University). Funded by Dizal Pharmaceuticals.
Key findings:
| Endpoint | Sunvozertinib | Chemotherapy | Effect size |
|---|---|---|---|
| Median PFS (BICR) | 10.3 months | 7.5 months | HR 0.65, p=0.0008 |
| 12-month PFS | 46.1% | 26.7% | — |
| ORR (BICR) | 68.1% | 35.4% | — |
| Median duration of response | 11.2 months | 7.1 months | — |
OS data remain immature at 38.9% maturity. OS curves crossed mid-trial; the investigators attribute this to early non-treatment-related deaths in the sunvozertinib arm and to 90.2% crossover from the chemotherapy arm to sunvozertinib upon progression. Safety was consistent with the established profile; no new signals were observed.
Clinical/research implication: EGFR exon20ins mutations occur in approximately 2–3% of all NSCLC cases and have historically been resistant to first-generation and second-generation EGFR inhibitors. Sunvozertinib was previously granted accelerated approval in the US and China for second-line exon20ins NSCLC; WU-KONG28 is the first positive phase 3 trial in this subtype in the first-line setting, and an NDA for first-line use has been accepted with Priority Review by China's NMPA. For cross-trial context: J&J's amivantamab plus chemotherapy (the Papillon regimen) reported an mPFS of 11.4 months and HR of 0.40 in a broadly similar first-line exon20ins population, with ORR of 67% — though the trials differ in design and patient selection, and head-to-head comparisons are not available. Heymach: "The WU-KONG28 trial marks a clinical turning point. The data demonstrate that a single-agent targeted oral regimen can deliver superior antitumor efficacy over conventional chemotherapy, offering a practice-changing alternative that may spare treatment-naïve patients from initial cytotoxic treatment." 9
Peer review status: Published in NEJM. Industry-funded (Dizal).
Note: A ~9 percentage-point discrepancy exists between ORR figures in the Dizal press release (68.1% labeled as Best Objective Response) and a secondary source citing 58.9% confirmed ORR from the NEJM paper. This likely reflects BOR vs. confirmed ORR definitions; the NEJM full text was inaccessible due to Cloudflare blocks at collection time, so both figures are noted here and the NEJM value should be used when full text becomes available.
5. ARB + CCB is the best-tolerated antihypertensive combination — and several combinations outperform placebo on side effects (JAMA network meta-analysis)
Journal: JAMA (IF ~63) · Network meta-analysis of randomized double-blind trials · Published May 28, 2026 (online) 10
Study design: A network meta-analysis of short-term randomized double-blind clinical trials evaluating adverse effects (AEs) and treatment discontinuation due to AEs for antihypertensive drugs and combinations. According to the accompanying JAMA editorial by JAMA Deputy Editor Mary McDermott and Stephen Persell, the analysis incorporated data from 716 trials. A separate count of 42 RCTs / 144,220 patients appears in secondary summaries; the precise scope of each count requires full-text confirmation. First author: Nelson Wang, BSc, MD, MPhil, PhD, FRACP (The George Institute for Global Health / UNSW / Imperial College London). Collaborators include Anthony Rodgers, Anushka Patel, Kazem Rahimi, Paul K. Whelton, and others.

Key findings:
- ARB + CCB ranked as the best-tolerated combination overall for adverse effects and treatment discontinuation. 11
- Four of the five best-tolerated regimens were combination therapies; four of those five contained an ARB.
- Several combination regimens demonstrated better tolerability than placebo — a threshold rarely crossed by individual drugs in prior meta-analyses, suggesting net symptomatic improvement (not merely tolerability parity). 11
- Proposed mechanism: RAAS inhibitors attenuate CCB-associated peripheral edema; certain combinations reduce headache, partially offsetting any increase in dizziness. 11
Clinical/research implication: The standard-of-care default across most guidelines has been to initiate antihypertensive therapy with monotherapy, escalating to combination only if target blood pressure is not reached. If combination therapy is both more effective at lowering blood pressure (established) and better tolerated than monotherapy (this paper's claim), the rationale for single-drug initiation weakens substantially. Wang: "In my view, these findings retire initial monotherapy as the default first-step treatment for hypertension." 11 The accompanying editorial flags a parallel problem: adverse effects are commonly misattributed to antihypertensives, leading to undertreatment. Clinicians managing patients on monotherapy who report side effects may have good reason to switch to an ARB+CCB combination rather than simplify to a different monotherapy or reduce dosing.
Limitations: Full text was not directly accessible at collection time (JAMA Cloudflare block); data here are sourced from the lead author's LinkedIn post and the accompanying editorial. A discrepancy in trial count (716 vs. 42) is unresolved.
Peer review status: Published in JAMA. Funding source not confirmed from available sources.
Cover image: AI-generated illustrative image (oncology laboratory setting).
参考ソース
- 1NEJM — Daraxonrasib or Chemotherapy in Previously Treated Metastatic Pancreatic Cancer
- 2StockTitan / Revolution Medicines — ASCO Plenary RASolute 302 press release
- 3NEJM — Teclistamab in Multiple Myeloma with One to Three Previous Lines of Therapy
- 4ecancer — ASCO 2026: Teclistamab extends survival, deepens remissions in relapsed multiple myeloma
- 5AJMC — Teclistamab as Monotherapy Shows Huge Advantage After First Relapse in Myeloma
- 6NEJM — Perioperative Apalutamide in High-Risk Localized Prostate Cancer
- 7GlobeNewswire / J&J — PROTEUS phase 3 prostate cancer study press release
- 8NEJM — First-Line Sunvozertinib in NSCLC with EGFR Exon 20 Insertion Mutations
- 9Dizal / PR Newswire — WU-KONG28 Phase 3 Results press release
- 10JAMA — Adverse Effects and Treatment Discontinuation of Blood Pressure–Lowering Drugs and Combinations: A Network Meta-Analysis
- 11LinkedIn — Nelson Wang: New Study Challenges Assumption on Blood Pressure Medication Tolerability
このコンテンツについて、さらに観点や背景を補足しましょう。