June 8–9 digest at a glance
Primary quantitative findings across the five papers
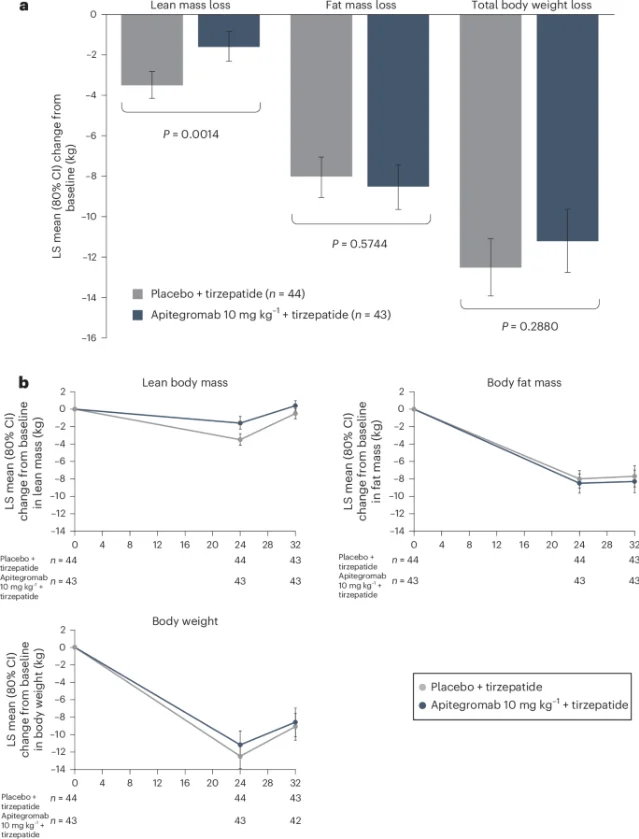
Five papers from June 8–9: apitegromab (EMBRAZE, Nature Medicine) preserves 54.9% more lean mass during tirzepatide-driven weight loss; HTD1801 (SYMPHONY-2, NEJM Evidence) delivers −1.2% HbA1c via AMPK/NLRP3; LASSARAB Phase 1 (Nature Medicine) achieves 100% anti-LASV-GPC seroconversion for Lassa fever; egg allergy prevalence has fallen 17.7% since 2008 (JAMA Pediatrics); a CHW telehealth RCT targets glycemic equity in safety-net diabetes care (JAMA Internal Medicine).

Research Brief
likely confidence rather than confirmed. 2"HTD1801, with its unique dual mechanism around the AMPK-NLRP3 axis, demonstrated multiple benefits in the SYMPHONY-2 study, including superior and durable glycemic control, lipid reduction, attenuation of inflammation, and improvements in renal function."— Prof. Linong Ji, Director, Dept. of Endocrinology, Peking University People's Hospital 2
| Outcome | LASSARAB (all doses combined, n = 44) | Imovax control (n = 10) |
|---|---|---|
| SAEs through Day 61 | 0 | 0 |
| Grade ≥3 AEs | 0 | 0 |
| Local solicited AEs | 86.7–100% | 80% |
| Systemic AEs | 33.3–71.4% | 60% |
| LASV-GPC IgG seroconversion (≥4× rise, Day 61) | 100% (44/44) | 0% (0/10) |
| Rabies seroprotection (RFFIT ≥0.5 IU/mL, Day 61) | 100% all doses | 100% |
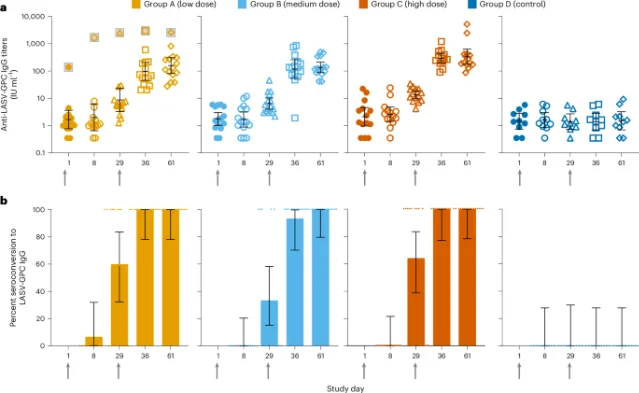
"These results provide the first clinical evidence that a rabies-vectored platform can safely generate immunity to Lassa virus in humans. The ability to combine protection against Lassa fever and rabies in a single vaccine could have a substantial public-health impact in regions where both diseases remain endemic."— Matthias J. Schnell, PhD, Director, Jefferson Center for Vaccines and Pandemic Preparedness, Thomas Jefferson University 4

"The field issued recommendations that outran the evidence, and families lived with the consequences. We owe families an honest accounting of that."
— Aaron E. Carroll, MD, and Ron Keren, MD, MPH 7
Add more perspectives or context around this Post.