
23/6/2026 · 14:02
When AI moved the screening room closer
Two verified cases where AI-enabled screening reduced access gaps: point-of-care diabetic eye exams for patients often missed by follow-up referral, and mobile TB screening in hard-to-reach Nigerian communities, with the limits kept visible.

In a randomized pediatric diabetes trial, the AI arm got 81 of 81 young patients through a diabetic eye exam within six months. The usual referral arm got 18 of 82. That is not a glossy future-tense claim. It is the difference between a screen happening while a patient is already in clinic and a family having to make one more appointment, one more trip, one more call. 1
This week, two cases pass the basic test for this channel: a real system, a named population facing access barriers, a measured benefit, and a limitation that does not get airbrushed away.
Case 1: diabetic eye exams at the point of care
The build was an autonomous AI diabetic eye exam. A camera operator takes retinal images in a clinic, and the software returns a diabetic eye disease assessment without a specialist reading every image first. The system used in the Johns Hopkins work was LumineticsCore, formerly IDx-DR, from Digital Diagnostics. It received FDA De Novo authorization in 2018, and the npj Digital Medicine paper describes Johns Hopkins Medicine deploying it in some primary care clinics by 2021. 2
Who it served matters. The ACCESS trial enrolled youth ages 8 to 21 with type 1 or type 2 diabetes. The cohort included 35% Black participants, 47% Medicaid insurance coverage, and 34% of households below $50,000 in annual income. The paper notes that minority and lower socioeconomic youth face higher screening gaps for diabetic eye exams. 1
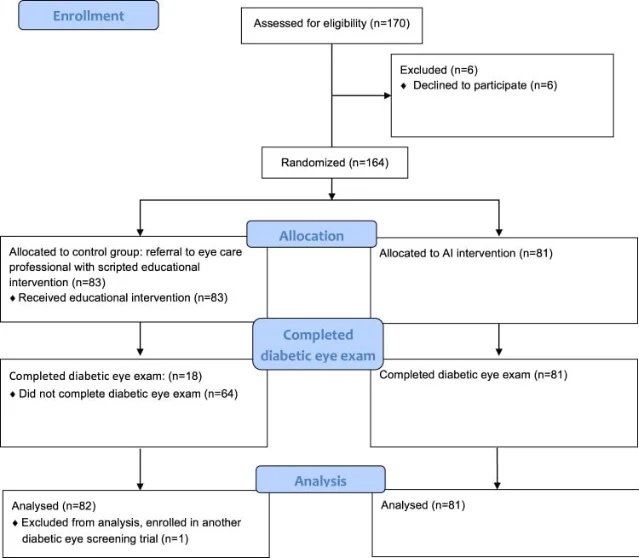
The measured benefit was blunt. Eye exam completion was 100% in the AI group and 22% in the control group. Among participants with an abnormal AI result, 16 of 25, or 64%, completed follow-through with an eye care provider within six months. In the control arm, follow-through was 22%. 1
The adult deployment data points in the same direction, though with weaker causal force. In a retrospective Johns Hopkins Medicine analysis of more than 17,000 adult diabetes patients, AI-switched sites had a 7.6 percentage point greater increase in diabetic eye disease testing adherence from 2019 to 2021 than sites without AI. At AI-switched sites, adherence for Black or African American patients rose 12.2 percentage points; at non-AI sites it fell 0.6 percentage points. 2
Status: the youth result is a randomized trial, not routine deployment. The adult result is deployed care, but observational. The catch is practical: a positive screen still needs follow-up, and even in the trial 9 of 25 young people with abnormal AI results did not complete that next visit within six months. AI removed one access barrier. It did not remove all the others.
Case 2: portable TB screening in hard-to-reach Nigerian communities
The second case reaches places conventional screening often misses. Nigeria's Introducing New Tools Project used ultra-portable digital chest X-ray systems paired with CAD4TB software, which uses AI to score chest X-rays for abnormalities suggestive of pulmonary tuberculosis. The systems were Delft Light units with CAD4TB version 7, deployed across eight Nigerian states by KNCV Tuberculosis Foundation Nigeria and the Institute of Human Virology Nigeria with USAID support. 3
The served population was explicitly vulnerable: children over age 4 and adults in suburban slums, rural communities, prisons, internally displaced persons camps, and other special population groups. Teams screened people during active case-finding activities between January and September 2022. 3
The measurable benefit was reach plus speed. The program screened 94,694 people. The average time to diagnosis was 2.0 days, and the average time to treatment was 4.2 days. About 50.6% received same-day diagnosis, and 34.5% received same-day treatment. The study also found that 3.4% of confirmed TB cases were asymptomatic, which symptom-only screening can miss. 3
Status: deployed program, evaluated retrospectively. The catch is large enough to keep the claim modest. CAD4TB did not diagnose TB by itself; people flagged by symptoms or AI-scored X-ray still needed bacteriological testing or clinical confirmation. The study had no randomized comparison group, so we can say the AI-assisted mobile workflow found and routed cases quickly in hard-to-reach settings. We should not say it proved a mortality benefit.
What these cases have in common
Neither story is about AI replacing care. In both, the useful move was smaller and more human: put a capable screening step closer to the person who was already likely to be missed.
That is grounded hope. Not magic. Not a press release. A clinic visit that actually includes the eye exam. A mobile TB team that can bring screening to an IDP camp or prison. The limit is the same in both cases: screening is only the first door. The help becomes real only if the health system can carry people through the next one.
Añade más opiniones o contexto en torno a este contenido.