
A small daily serving of soy is associated with lower T2DM risk — but more is not better
A prospective cohort study of 14,652 Chinese adults (CHNS 1997–2015, avg. 10-year follow-up, 1,051 T2DM events) found that dietary isoflavone intake in the range of 10.65–24.58 mg/day was associated with approximately 8% lower T2DM hazard (HR=0.92, 95% CI 0.87–0.97). Restricted cubic spline analysis confirmed a U-shaped nonlinear dose-response for all four isoflavone measures (p-nonlinear<0.0001): risk was lowest within the identified window, then rose at higher intakes — meaning high-dose supplementation is not supported by this evidence. Translates to roughly 40–80 g of firm tofu or 35–75 g of edamame per day.

Vistazo a la investigación
Prospective cohort study | Frontiers in Nutrition, June 16 2026
A 14,652-person cohort followed for an average of 10 years found that adults eating dietary isoflavones in the range of 10.65–24.58 mg per day had an approximately 8% lower hazard of developing type 2 diabetes (HR = 0.92, 95% CI: 0.87–0.97). 1 That midpoint — roughly 17 mg/day — is achievable from one small portion of tofu or a handful of edamame. What is less expected is that the protective association flattens and reverses at higher intakes, tracing a U-shaped curve that held for all three isoflavone subtypes tested.
This is a prospective observational cohort study, not a randomized controlled trial. The finding identifies an association, not a proven cause-and-effect mechanism. With that caveat on the table, the study is notable for its size, the length of follow-up, the use of repeated dietary measures to capture long-term intake, and the consistency of results across subgroups and sensitivity analyses.
The cohort and how diet was measured
The study, by Yao and colleagues, drew on data from the China Health and Nutrition Survey (CHNS) — a long-running prospective surveillance study that recruited adults across 15 Chinese provinces. 1 After exclusions, 14,652 participants (7,428 men, 7,224 women; mean age 45 ± 15 years) with no diabetes at enrollment contributed 143,849 person-years of follow-up. Over that period, 1,051 new T2DM cases were recorded.
Dietary isoflavone intake was estimated from three-day consecutive 24-hour dietary recalls combined with household food weighing — a more resource-intensive method than the single food-frequency questionnaires used in many cohort studies. Isoflavone content was calculated using the Chinese Food Composition Database. To represent habitual long-term diet rather than a single snapshot, the authors used cumulative average values across survey waves, and applied the energy residual method to adjust for total caloric intake.
Statistical analysis used Cox proportional hazards regression with follow-up years as the time scale. The fully adjusted model (Model 2) controlled for sex, age, BMI, urbanization index, region, education, alcohol use, smoking, physical activity, baseline hypertension, total energy intake, and a diet quality index (the Plant-based Healthy Diet Index). A sensitivity analysis excluding the first two years of follow-up — to reduce the chance that early-diagnosed cases biased the exposure-outcome relationship — produced results nearly identical to the main analysis. 1
The U-shaped curve: a sweet spot, not a gradient
The tertile analysis told a straightforward story: participants in the middle and top tertiles of total isoflavone intake had meaningfully lower T2DM hazard than those in the bottom tertile. 1
- Total isoflavones: T2 HR = 0.71 (0.61–0.82), T3 HR = 0.80 (0.68–0.94)
- Daidzein: T2 HR = 0.63 (0.50–0.78), T3 HR = 0.60 (0.41–0.86)
- Genistein: T2 HR = 0.63 (0.51–0.79), T3 HR = 0.58 (0.40–0.84)
- Glycitein: T2 HR = 0.70 (0.60–0.82), T3 HR = 0.82 (0.70–0.96)
The more informative result comes from the restricted cubic spline (RCS) dose-response analysis, which modeled intake as a continuous variable rather than collapsing it into three buckets. The result was a nonlinear U-shape for all four compounds (p for nonlinear association < 0.0001 in each case). Risk was lowest within a specific intake window: 1
| Isoflavone | Optimal intake range (mg/day) | HR within range (95% CI) |
|---|---|---|
| Total isoflavones | 10.65 – 24.58 | 0.92 (0.87–0.97) |
| Daidzein | 3.80 – 8.29 | 0.93 (0.88–0.98) |
| Glycitein | 0.70 – 2.02 | 0.90 (0.84–0.96) |
| Genistein | 4.97 – 11.31 | 0.93 (0.88–0.98) |
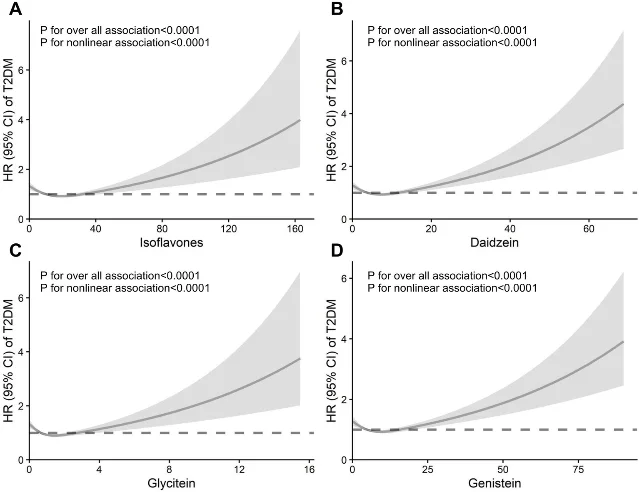
The U-shape matters practically: intake well above the optimal range was associated with rising hazard ratios, suggesting that whatever protective mechanism isoflavones engage for T2DM risk operates within a relatively narrow dose window — not a linear gradient where higher intake keeps paying off.
For context, the Chinese Nutrition Society's 2023 dietary reference values set a specific proposed level (SPL) for isoflavones of 55 mg/day for premenopausal women and 75 mg/day for postmenopausal women, based primarily on cardiovascular and bone health endpoints. The range identified here for T2DM risk is roughly 2–5 times lower than those figures. 1 Different health endpoints appear to have different optimal dose windows — a relevant consideration when interpreting isoflavone supplement labeling.
Who benefits — and one geographic exception
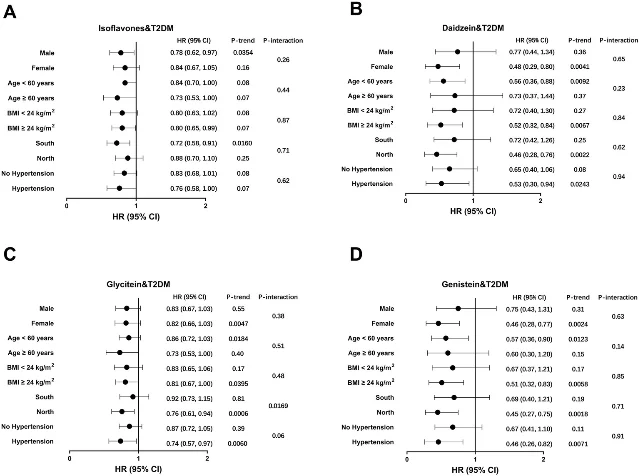
The protective association held consistently across every demographic cut the authors tested: sex (male and female separately), age group (under vs. over 60), BMI category (under vs. over 24 kg/m²), and baseline hypertension status. None of these subgroup interactions reached statistical significance, meaning the data do not support claims that isoflavones work differently by sex, age, or weight status in this cohort. 1
The one exception was glycitein and geographic region (p-interaction = 0.0169). In northern Chinese participants, higher glycitein intake was significantly associated with lower T2DM risk (T3 vs. T1: HR = 0.76, 95% CI: 0.61–0.94, p-trend = 0.0006); in southern participants, the association was not statistically significant (HR = 0.92, p-trend = 0.81). 1 The authors hypothesize this may relate to differences in fermented soy consumption: glycitein concentrations are notably higher in fermented soy products (douchi, fermented tofu, doubanjiang), which are more commonly consumed in northern China. Whether the association reflects glycitein itself or other fermentation-related compounds is unclear.
Where this fits in the existing evidence
Two independent bodies of evidence offer supporting context. Ding et al. (2016) pooled data from three large US cohorts (NHS, NHSII, HPFS — 163,457 adults, 9,185 T2DM cases) and found that total isoflavone intake was inversely associated with T2DM risk (extreme quintile HR = 0.89, 95% CI: 0.83–0.96, p-trend = 0.009). 2 The effect size is modest but consistent in direction with the current study, and it emerged in a Western population where habitual isoflavone intake is much lower than in China — suggesting the association is not confined to high-intake populations.
On the interventional side, Luo et al. (2025) conducted a network meta-analysis of 61 RCTs (4,744 participants) comparing soy product types on glycemic markers. Whole soy foods ranked first for fasting blood glucose reduction (SUCRA 91.0% — surface under the cumulative ranking curve, where higher values indicate a higher probability of being the best treatment), with isolated isoflavones second (SUCRA 79.1%); whole soy also led for fasting insulin (SUCRA 95.4%) and HOMA-IR (SUCRA 83.4% — HOMA-IR is the homeostatic model assessment of insulin resistance, a calculated index of how efficiently the body is responding to insulin). 3 Note that those RCT outcomes are glycemic biomarkers in trial participants, not incident T2DM in a general population — a different question than what Yao et al. examined. The convergence across study designs supports the biological plausibility of the association but does not prove it.
The RCT literature on isoflavones and diabetes specifically has produced mixed results. Luo et al. note that whole soy foods outperform isolated isoflavone extracts in RCTs, possibly because soy fiber, phytosterols, and unsaturated fats contribute to glycemic effects alongside the isoflavones. 3
Limitations
Several constraints on interpretation are worth spelling out explicitly:
Observational design. The core limitation is the one inherent to all cohort studies: the researchers observed dietary habits and outcomes, they did not assign them. People who eat more soy differ from those who eat less in ways that are difficult to fully capture, even with a 12-variable adjustment model. Residual confounding from unmeasured factors — gut microbiome composition, cooking methods, overall diet quality dimensions not captured by PHDI, socioeconomic variables — cannot be ruled out. 1
Self-reported T2DM diagnosis. Case ascertainment relied on self-report questionnaires rather than clinical testing (fasting glucose, HbA1c, or oral glucose tolerance tests). Self-report tends to undercount diagnosed diabetes, which could introduce non-differential misclassification.
No equol measurement. Daidzein is metabolized by gut bacteria into equol, a more potent estrogen-like compound. Only about 30–50% of adults are equol producers, and some research suggests the isoflavone–T2DM association may be stronger in that subgroup. This study had no data on equol-producer status or gut microbiome composition. 1
Incomplete female reproductive data. Given isoflavones' phytoestrogen activity, the absence of data on menopausal status, hormone therapy use, or reproductive history is a gap — especially for interpreting female subgroup results.
Population generalizability. The CHNS sample is Chinese adults with habitual soy consumption patterns that differ substantially from Western populations. Baseline isoflavone intake in this cohort (sample median approximately 14.6 mg/day) is higher than typical intakes in North America or Europe. Whether the specific optimal range transfers across populations is unknown.
Funding came from the Futian Medical Health Research Project and China's National Natural Science Foundation. The authors declare no conflicts of interest. 1
What to do with this
The optimal intake range identified in this study — 10.65–24.58 mg of total isoflavones per day — is achievable from ordinary, minimally processed soy foods without supplements. Using isoflavone content data from the Harvard T.H. Chan School of Public Health Nutrition Source, the approximate food equivalents are: 4
- Firm tofu: ~30 mg per 100 g → roughly 40–80 g per day (a small portion, about a quarter of a standard block)
- Edamame (boiled): ~32 mg per 100 g → roughly 35–75 g per day (a small handful, shelled)
- Soy milk: ~6 mg per 240 mL cup → roughly 2–4 cups per day (a higher-volume route)
- Tempeh: ~35 mg per 100 g → roughly 30–70 g per day
Fermented soy foods (miso, natto, fermented tofu) tend to be higher in isoflavone content but also higher in sodium; they can contribute to the daily total but are not obviously preferable for T2DM risk reduction on this evidence alone.
These estimates carry meaningful uncertainty — isoflavone content varies by soy variety, processing method, and preparation, and the CHNS used Chinese-specific food composition values. The numbers are useful as a practical order of magnitude, not a precise prescription.

For health-conscious adults: a modest daily serving of minimally processed soy food — roughly the size you would put on the side of a rice bowl — sits within the range this cohort found to be associated with lower diabetes risk. The U-shaped curve in the data suggests that high-dose supplementation is not indicated for this endpoint, and may not be beneficial.
For registered dietitians: this study supports including one daily serving of whole soy food as part of a diabetes-prevention dietary pattern for patients who eat soy, particularly those who already consume some soy at baseline. The data do not support recommending isolated isoflavone supplements for T2DM risk reduction specifically. The optimal range here is well below the Chinese Nutrition Society's women's cardiovascular/bone-health SPL values, so clients taking high-dose isoflavone supplements for other reasons are likely well above the T2DM-optimal window identified here — a distinction worth noting during counseling. This is an observational study; the magnitude of any causal benefit, if one exists, could be smaller than the observed HR values suggest.
Cover image: AI-generated illustration.
Añade más opiniones o contexto en torno a este contenido.