Prosopagnosia: What Face Blindness Reveals About the Brain's Dedicated Face Module
Prosopagnosia — face blindness — is the strongest neuropsychological evidence that face recognition is a functionally distinct module in the brain. This article covers the two forms (acquired and developmental), the double dissociation argument that separates face recognition from general visual cognition, what lesion anatomy reveals about the processing cascade, the face-specificity debate, and the discovery of super-recognizers at the other end of the distribution.

Picture walking into a party and realizing that none of the people you see, however well you know them, look familiar. Not because of darkness, or alcohol, or distraction — but because the neural circuit that makes faces mean something is simply broken. You see eyes, a nose, a mouth arranged normally. You can tell it's a face. You just cannot tell whose face it is.
This is prosopagnosia, colloquially called face blindness. It is not as rare as it sounds, and it has taught us more about how the brain organizes cognition than almost any other neurological syndrome.
A name coined from wounded soldiers
The term prosopagnosia was introduced in 1947 by the German neurologist Joachim Bodamer, who described three patients with selective impairment in recognizing faces — two of them soldiers injured in World War II 1. The word comes from the Greek prosopos (face) and agnosia (absence of knowledge). But face recognition problems had been described at least 150 years earlier; what Bodamer gave the field was a name sharp enough to generate a research program 2.
The modern study of prosopagnosia took off in the second half of the twentieth century as single-patient case studies accumulated. What they kept revealing, again and again, was a strange dissociation: a person whose general intelligence is intact, whose vision for objects and scenes is intact, whose memory is intact — yet who cannot recognize a face they have seen hundreds of times.
Two forms with very different origins
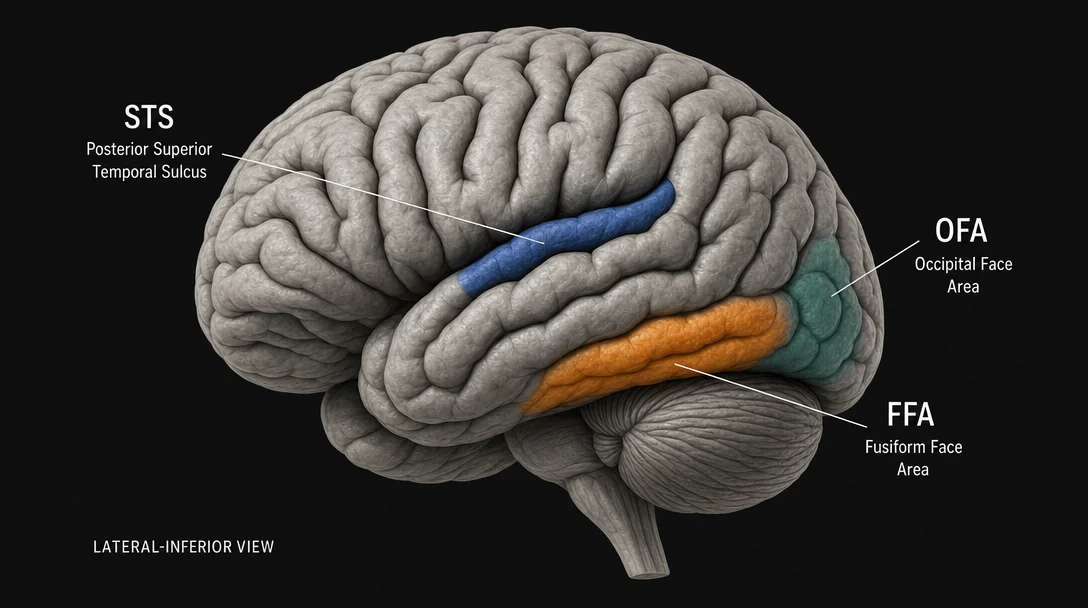
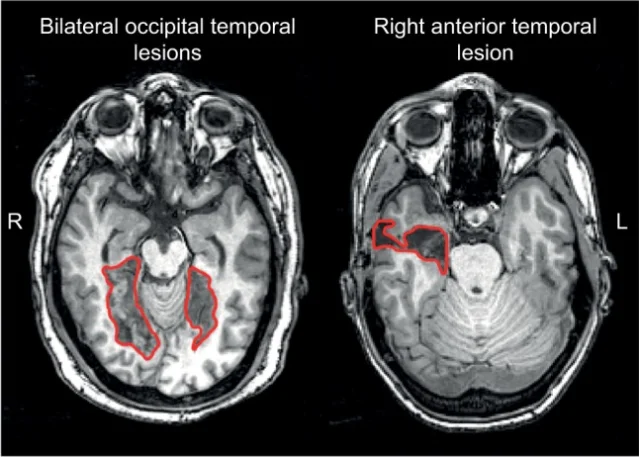
Acquired prosopagnosia results from brain damage. Stroke, traumatic injury, encephalitis, tumors, and temporal-lobe surgery can all produce it. The lesions most commonly involve the right hemisphere, particularly the occipitotemporal cortex — the region where the fusiform face area (FFA), introduced in the previous article in this series, resides 2. When the lesion is right-hemisphere only, the result is typically the apperceptive variant — the patient cannot encode the structural details of faces accurately. When damage extends to the anterior temporal cortex (especially bilaterally), the result leans toward the associative variant — faces can be structurally perceived but cannot be matched to stored identity representations.
Developmental prosopagnosia (DP) is an entirely different story. These individuals have never been able to recognize faces well. There is no brain injury, no obvious structural lesion on standard MRI, no general intellectual or memory problem. Yet they consistently score far below average on every standardized face recognition test 2.
How common is DP? The often-quoted figure of 2–2.5% came from a 2006 study by Kennerknecht et al. using questionnaire-based diagnosis. A more rigorous 2023 study from Harvard Medical School, led by Joseph DeGutis, administered both objective face recognition tests and self-report questionnaires to a web-based sample of 3,116 adults. Depending on the diagnostic stringency applied, estimated prevalence ranged from 0.13% to 5.42%, with the most commonly used research criteria yielding about 0.9–2% 3. That cluster of methodological variance is itself informative: it means DP is not a clean categorical diagnosis but something closer to the low tail of a continuous distribution of face recognition ability.
DP runs in families. Some pedigrees show as many as ten affected members across two generations, suggesting a heritable component 2. The broader picture of face recognition ability in the general population is also heritable — monozygotic twins are substantially more similar in face recognition performance than dizygotic twins — pointing to a genetic basis for individual differences across the entire distribution, not just at the impaired extreme.
The double dissociation argument
The phrase "double dissociation" appears constantly in the prosopagnosia literature. It describes a logical structure: if damage to area A impairs function X but not function Y, and damage to area B impairs function Y but not function X, you have strong evidence that X and Y are cognitively and neurally distinct.
For faces, the classic double dissociation contrasts prosopagnosia with visual agnosia. Patients with prosopagnosia fail to recognize faces but can usually identify everyday objects normally. Patients with visual agnosia (damage to a different set of regions) lose the ability to identify common objects but may retain face recognition 4. MIT 9.13 uses this exact contrast as a pivotal lecture in the face-processing module.
This dissociation is the strongest neuropsychological argument that face perception is not just a subset of general visual expertise applied to a particular object category. If face recognition and object recognition were drawing on exactly the same machinery, you could not get one without the other. The double dissociation says you can.
What the lesion tells you about the network
Acquired prosopagnosia turned out not to be a single disorder. A 2016 review by Corrow, Dalrymple, and Barton synthesized functional MRI and lesion evidence to show that lesion location predicts the type of deficit 2:
- Damage to occipitotemporal cortex (including the FFA and occipital face area, OFA) produces the apperceptive variant — structural face encoding fails. Patients cannot judge whether two faces are the same person even when looking at them simultaneously.
- Damage to anterior temporal cortex produces the associative variant — structural encoding may be intact, but faces cannot be matched to stored identity. A patient can see that two photographs show the same face yet have no sense of who that person is.
The Bruce and Young cognitive model (1986), which divides face processing into face encoding → face recognition units → person identity nodes → name generation, maps reasonably well onto this anatomical gradient: earlier (posterior) damage disrupts encoding; later (anterior) damage disrupts identity access 2.
One practical consequence: topographic disorientation — getting lost in familiar environments — accompanies acquired prosopagnosia in roughly 29% of cases 2. The likely reason is anatomical proximity: the parahippocampal place area (PPA), covered in the previous article in this series, sits immediately adjacent to the FFA in the occipitotemporal cortex. Lesions that take out face processing often nick scene and navigation processing too.
The face-specificity debate
Prosopagnosia's relationship to "face specificity" is genuinely contested. The clean version of the story — prosopagnosia is a deficit in faces alone, because faces are processed by a dedicated module — is not quite what the data show.
Studies of both acquired and developmental prosopagnosia turn up cases where recognition deficits extend to other object categories, particularly those the patient had high prior expertise in (e.g., cars for car enthusiasts) 2. This is the expertise hypothesis in mirror image: if the FFA is partly a general expert-object recognizer that faces happen to dominate, then losing it should impair recognition of other high-expertise categories too. The data support this, at least in some patients.
The majority of prosopagnosics, however, show deficits far more pronounced for faces than for other objects, especially in developmental cases where four out of six children in one study showed face-specific impairment 2. The most defensible current position is probably this: face processing relies on a system that is biased toward faces from very early in development, that overlaps partially with high-expertise object recognition, but that has a face-specific component not fully shared with any other category. Prosopagnosia is the cost of having that system.
Super-recognizers: the other end
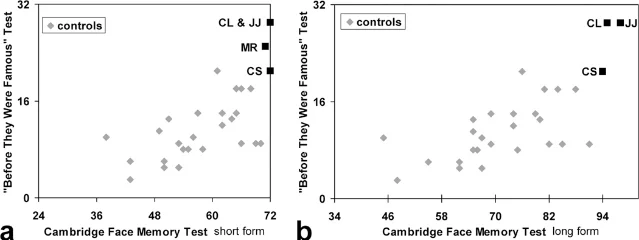
In 2009, Russell, Duchaine, and Nakayama published a paper that changed the framing of the whole field. They tested four people who had volunteered after media coverage of prosopagnosia research, claiming to have extraordinary face recognition ability. All four were confirmed to be dramatically better than any control subject on two independent tests: the "Before They Were Famous" (BTWF) test (recognizing famous people from childhood photos before they became recognizable) and the Cambridge Face Memory Test (CFMT) 5.
The paper called these individuals super-recognizers. Their scores on both tests fell entirely outside the control range — not at the ceiling, but beyond it. On tests specifically designed to be too difficult for ordinary face recognition, they still scored well above controls.
The inversion effect data were equally telling: super-recognizers showed a larger face inversion effect than controls, who in turn showed a larger effect than developmental prosopagnosics. The inversion effect — the finding that faces are recognized much worse upside-down than other objects — is a marker of holistic face processing, the tendency to process a face as a unified whole rather than as a collection of features. The gradient in inversion effect size across these three groups directly links face recognition ability to the degree of holistic processing.
The practical implication extends beyond the lab. Super-recognizers have been deployed by the Metropolitan Police in London to identify suspects from CCTV footage, with performance substantially better than automated facial recognition software in some conditions. The distribution of face recognition ability that prosopagnosia research opened up turns out to have real applications at both ends.
What we still don't know
Three open problems are worth flagging:
The neural basis of DP remains unclear. Standard structural MRI typically looks normal. Diffusion tensor imaging studies suggest subtle abnormalities in white-matter connectivity within the face-processing network, but findings are not consistent across labs 2. Whether DP reflects a connectivity problem, an early developmental failure of the FFA to become face-selective, or something else is unresolved.
Is face recognition ability truly a continuum, or is there a categorical disorder? DeGutis et al.'s 2023 cluster analysis of 3,116 participants failed to find a natural cluster of poor face recognizers that would justify a clean categorical diagnosis 3. The data look more like a continuous distribution with no obvious breakpoint. This mirrors the debate around dyslexia: is it a discrete disorder or the low tail of reading ability?
How much does the deficit extend to other people-recognition channels? Most prosopagnosics eventually compensate to some degree using voice, gait, hairstyle, or context. Only a minority have parallel deficits in voice recognition, and that minority tends to have bilateral anterior temporal lesions affecting the "person identity node" rather than the face-specific encoding stage 2. The architecture separating face identity from person identity turns out to be empirically tractable — and prosopagnosia is how we know it exists.
Landmark paper: Corrow, S.L., Dalrymple, K.A., & Barton, J.J.S. (2016). Prosopagnosia: current perspectives. Eye and Brain, 8, 165–175. DOI: 10.2147/EB.S92838 2
Also foundational: Bodamer, J. (1947). Die Prosop-Agnosie. Archiv für Psychiatrie und Nervenkrankheiten, 179(1–2), 6–54. [Bodamer 1947 — the naming paper, not publicly accessible in full; historical summary in Josephs 2024 1]
And: Russell, R., Duchaine, B., & Nakayama, K. (2009). Super-recognizers: People with extraordinary face recognition ability. Psychonomic Bulletin & Review, 16(2), 252–257. DOI: 10.3758/PBR.16.2.252 5
Course connection: MIT 9.13 The Human Brain (Nancy Kanwisher) — Lecture 2.14: Double Dissociations (Prosopagnosia vs. Agnosia), and the adjacent module on individual differences in face recognition and developmental prosopagnosia. See 4 and Individual differences in face recognition and developmental prosopagnosia.
Fuentes de referencia
- 1Josephs 2024, Brain Communications — Prosopagnosia history
- 2Corrow et al. 2016, Prosopagnosia: current perspectives — PMC
- 3DeGutis et al. 2023, What is the prevalence of developmental prosopagnosia? — PMC
- 4MIT Nancy's Brain Talks — 2.14 Double Dissociations: Prosopagnosia vs. Agnosia
- 5Russell, Duchaine & Nakayama 2009, Super-recognizers — PMC
Añade más opiniones o contexto en torno a este contenido.