
Oat fiber cut glucose spikes 13% — with a catch
Oat fiber cut peak glucose 13% in 2 weeks. Strong COI: all 5 authors are manufacturer employees. GI tolerance data is the cleaner takeaway.

Vistazo a la investigación
A depolymerized short-chain oat β-glucan (marketed as one.bio Oat Fiber, or "scOat Fiber") reduced peak post-meal glucose by roughly 22 mg/dL — about 13% — after two weeks of 20 g/day supplementation in healthy adults. The fiber also showed a clean GI tolerance profile across all three doses tested: 5, 10, and 20 g/day.
Those are the headline numbers from Marcobal et al. (2026), published June 10, 2026 in Frontiers in Nutrition. 1 Before going further: all five authors are employees of One Bio Inc., the Sacramento-based company that manufactures and sells this fiber. The study was funded entirely by One Bio. There is no independent third-party replication yet. That single fact changes how every number in this article should be read.
What makes this fiber different from ordinary oats
Standard oat β-glucan is a high-molecular-weight fiber found naturally in oats. It lowers post-meal glucose primarily by increasing the viscosity of digested food in the gut — slowing gastric emptying, trapping glucose, and blunting the spike. This mechanism is recognized by the FDA and European Food Safety Authority (EFSA) and is backed by decades of RCT evidence. 1
scOat Fiber is made by controlled depolymerization of that same high-molecular-weight β-glucan — cutting it into short oligosaccharide chains of 3 to 30 monomer units. The result: 91.3% oat fiber content (90.4% β-glucan) but with much lower viscosity and far higher solubility than conventional oat fiber. It dissolves fully in water or food without thickening. Because it cannot rely on viscosity, it would have to work through different mechanisms if it works at all.
One Bio's own in vitro research (Marcobal et al. 2024, Nutrients) suggested three potential mechanisms: inhibition of α-glucosidase (slowing starch digestion), inhibition of SGLT1 transporters (reducing intestinal glucose absorption), and fermentation by gut microbiota into short-chain fatty acids (SCFAs) like butyrate, propionate, and acetate. 2 Those are plausible pathways. They are also, again, from the same research group. The new human trial is the first test of whether any of this actually happens in people — and it is not a placebo-controlled RCT.
What the trial found
Study design: 63 healthy adults (67 enrolled, 4 withdrew) were assigned sequentially — not randomly — to three dose groups: 5, 10, or 20 g/day of scOat Fiber dissolved in water for two weeks. The study was open-label with no placebo arm. Participants wore a Dexcom G6 Pro continuous glucose monitor (CGM) throughout. Post-meal glucose was assessed with a standardized rice challenge eaten at home (unsupervised). The trial ran from January to April 2025 (NCT06739941). 1
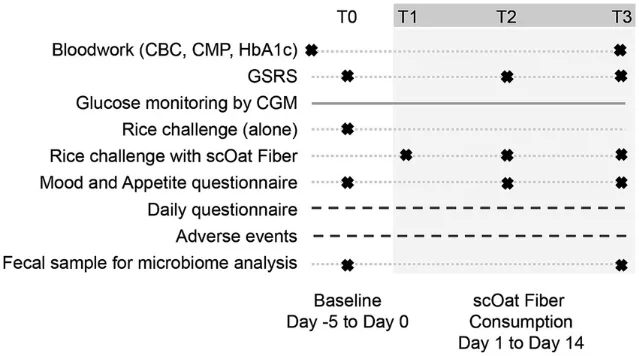
The primary outcome was gastrointestinal tolerance, measured by the Gastrointestinal Symptom Rating Scale (GSRS). Glucose was a secondary and exploratory outcome, not the primary pre-specified endpoint. That distinction matters: glucose was not what this trial was designed to prove.
GI tolerance results (primary, most reliable):
| Dose | GSRS change | Abdominal pain | Constipation |
|---|---|---|---|
| 5 g/day | Significantly improved (p = 0.0012) | Improved (p = 0.0005) | No change |
| 10 g/day | Significantly improved (p = 0.0105) | Improved (p = 0.0074) | Reduced (p = 0.0244) |
| 20 g/day | No significant change (p = 0.6328) | No change | No change |
All three dose groups stayed within the low-to-mild range throughout — no group got worse. Reported adverse events were transient and non-dose-limiting: bloating (n = 26), abdominal distension (n = 15), constipation (n = 13), abdominal pain (n = 7), and diarrhea (n = 5). One participant withdrew, but was concurrently taking the antiemetic ondansetron (Zofran), making causality unclear. For comparison, other commonly used fibers — inulin, polydextrose, resistant maltodextrin — typically produce measurable GI discomfort at doses of 5–7.5 g/day. scOat Fiber was well tolerated even at 20 g/day. 1
Glucose results (secondary and exploratory, n = 38 of 63; 25 excluded due to missing CGM data or non-fasting status):
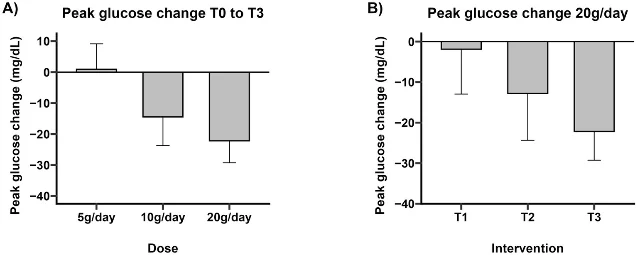
- 20 g/day: Peak glucose fell from 166.3 → 144.2 mg/dL (p = 0.018, −13%). Glucose spike height fell from 61.5 → 41.9 mg/dL (p = 0.024, −32%). 83% of participants in this group showed a reduction.
- 10 g/day: Peak glucose fell from 174.2 → 159.7 mg/dL (p = 0.023, −8%). Spike height non-significant.
- 5 g/day: No significant change in peak glucose.
Glucose variability (time in range, standard deviation) also improved at 10 and 20 g/day:
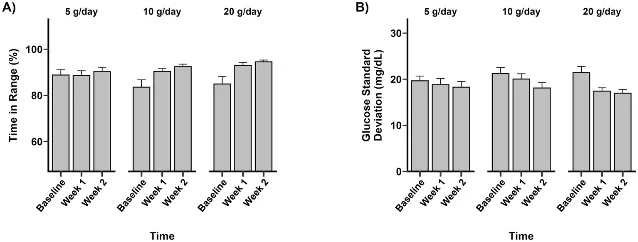
At 20 g/day, glucose SD fell from 21.4 to 17.0 mg/dL (p = 0.0003). Neither dose produced significant changes in the integrated area under the glucose curve (iAUC or total AUC) — only the peak and spike shape changed. No endpoint HbA1c or fasting glucose laboratory measurement was collected; all glucose data comes from CGM.
How much to trust these numbers
The glucose findings are dose-dependent, which is harder to explain away as coincidence than a single positive result. The authors appropriately applied false discovery rate correction. The study was conducted by People Science Inc. (Los Angeles), a third-party clinical research organization, with an independent IRB (Advarra), and the paper is peer-reviewed and open-access.
Those are genuine strengths. But the limitations are substantial enough that the glucose data should be treated as hypothesis-generating, not confirmatory.
No randomization: Participants were assigned sequentially by enrollment order, not by chance. The 5 g/day group had a significantly higher baseline GSRS score (p = 0.019), which means group composition was not balanced from the start — a textbook consequence of non-random allocation. 1
No placebo control: The researchers acknowledge this openly. As they write, "The open label design and lack of a placebo control limit the ability to distinguish intervention effects from placebo effects, particularly for subjective outcomes such as mood and sleep." 1 Glucose measured via CGM is less susceptible to placebo effects than GSRS scores, but behavioral changes (eating more carefully at the rice challenge because participants knew they were in a study) could still influence peak glucose independent of the fiber.
~40% of glucose-eligible participants excluded: 25 of 63 evaluated participants were removed from the glucose analysis: missing CGM data (n = 15), no baseline recording (n = 6), non-fasting status (n = 2), and timing errors at the rice challenge (n = 2). The rice challenge was self-administered at home without supervision. An approximately 40% exclusion rate in the analysis subset introduces selection bias that is difficult to quantify.
Healthy adults only: All participants had HbA1c below 6.5% with no metabolic disease or gastrointestinal conditions. People with prediabetes, type 2 diabetes, or obesity were explicitly excluded. The population that most needs post-meal glucose management was not studied. 1
All authors work for the manufacturer: This is the critical issue — and it is not a technicality. One Bio's CSO Matthew Amicucci is a co-author and the company's founder. The other four authors (Angela Marcobal, Katharine Ng, Riley Drexler, Bruce McConnell) are company employees. One Bio funded the study, manufactures the product, and sells a consumer brand (GoodVice) built around the same fiber. The paper states funders had no involvement in design or analysis. That may well be true. There is simply no independent way to verify it, because there is no independent oversight. 1 3
ClinicalTrials.gov discrepancies: The registered trial title was "Investigating the Tolerability of Oat Fiber (BG-OS) in Healthy Individuals" — no mention of glucose regulation. The published title adds "regulates glucose metabolism." The registration recorded 60 participants; the paper reports 67 enrolled. Additional glucose variability endpoints (TIR, SD, iTIR) appeared in the published paper but were not pre-specified in the registration. 4 These changes could reflect legitimate protocol evolution in a pilot study, but they also fit a pattern of expanding scope toward significant results after the fact.
The actionable takeaway
Split by what the evidence actually supports at this stage:
GI tolerance (5–10 g/day): lower risk to act on. The primary endpoint was GI tolerance, and the trial found a clear benefit at 5 and 10 g/day — improving abdominal pain and constipation without the bloating or gas that makes inulin or resistant starch supplements hard to stick with. This finding holds even accepting the study's design limitations, because GI tolerance was the pre-specified primary outcome, both doses showed improvement, and GI response is less susceptible to expectation bias than mood or energy. For adults who want more dietary fiber but find conventional fiber supplements poorly tolerated, 5–10 g/day of a soluble, low-viscosity β-glucan-based supplement is a reasonable thing to try, with the usual caveat that the supporting evidence comes from one industry-funded pilot.
Post-meal glucose (20 g/day): wait for independent replication. The 13% reduction in peak glucose at 20 g/day is the kind of signal worth watching — dose-dependent, statistically significant, biologically plausible. But it comes from a non-randomized, unblinded, manufacturer-run pilot study where about 40% of the glucose-eligible participants were excluded from analysis, and the population was healthy adults without any glucose dysregulation. None of the prior evidence base for conventional oat β-glucan applies here, because the mechanism is entirely different and the depolymerized form is a distinct ingredient. The authors themselves call for "future randomized controlled trials… to confirm these findings." 1 That is the right call. Until an independent RCT with a placebo arm and a population that actually has glucose dysregulation replicates this result, recommending 20 g/day specifically for glucose management is premature.
For dietitians: Clients asking about this study — or about the GoodVice shakes ($4.85–$5.71/day for 10 g of fiber plus 20 g protein) — can be told the GI tolerance data is more solid than the glucose data, the glucose data is intriguing but not yet independently confirmed, and the product being studied and the product being sold are not identical (the clinical trial used pure scOat Fiber powder dissolved in water, not a protein shake). If a client has early-stage glucose concerns, the existing evidence base for conventional high-molecular-weight oat β-glucan from whole oats or oat bran — supported by decades of independent RCTs and recognized by EFSA and FDA — remains the stronger recommendation. 2
One thing to watch: the research team collected stool samples during the trial for microbiome and SCFA analysis. Those results have not been published yet. If gut microbiota composition shows meaningful change at the doses where glucose improved, that would add mechanistic support and shift the evidential weight. For now, the mechanism remains an inference. 1
Bottom line: 20 g/day of scOat Fiber cut peak post-meal glucose by 13% over two weeks — a signal from a pilot study that deserves independent replication, not clinical adoption. The GI tolerance story is the one with cleaner evidence and a clearer immediate use case.
Cover image: AI-generated illustration.
Añade más opiniones o contexto en torno a este contenido.